

High-Dose Chemotherapy and Blood Autologous Stem-Cell Rescue Compared With Standard Chemotherapy in Localized High-Risk Ewing Sarcoma: Results of Euro-E.W.I.N.G.99 and Ewing-2008
- PMID: 30188789
- PMCID: PMC6209090
- DOI: 10.1200/JCO.2018.78.2516
High-Dose Chemotherapy and Blood Autologous Stem-Cell Rescue Compared With Standard Chemotherapy in Localized High-Risk Ewing Sarcoma: Results of Euro-E.W.I.N.G.99 and Ewing-2008
Abstract
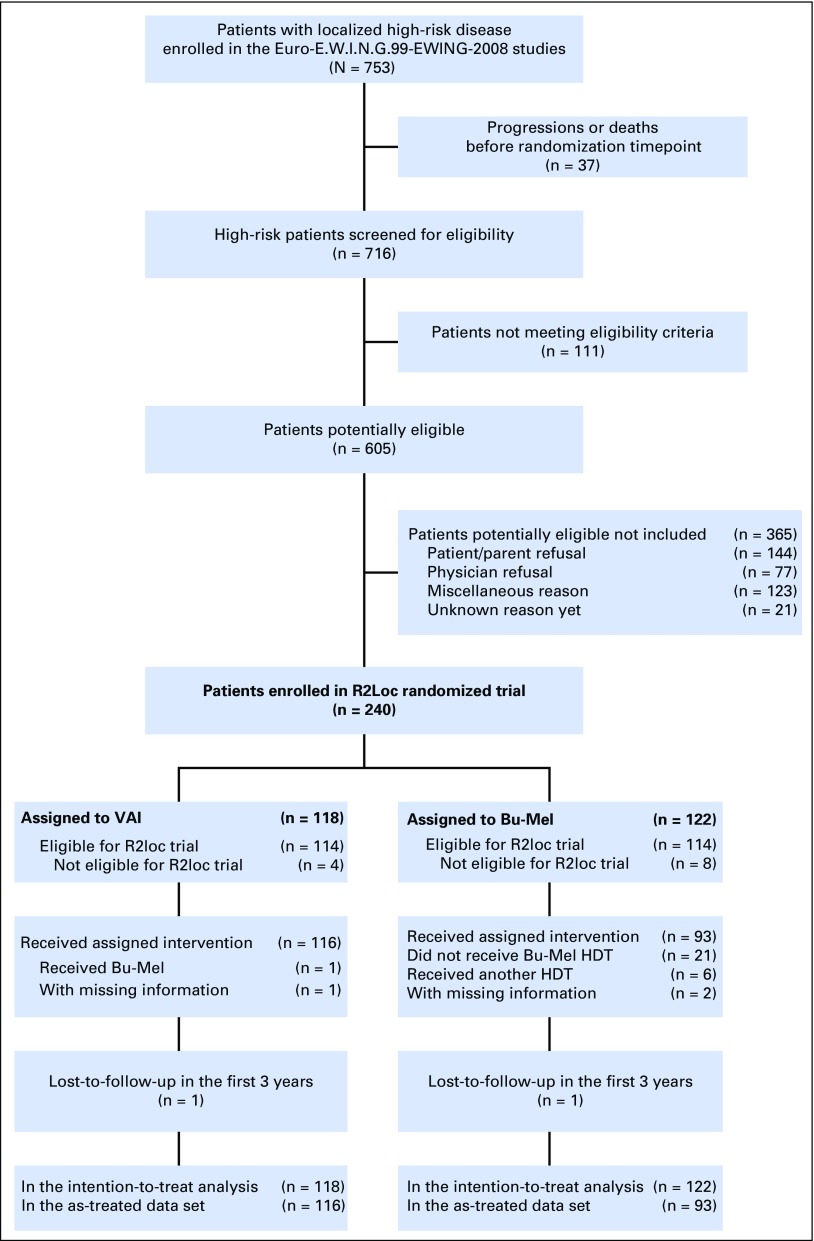
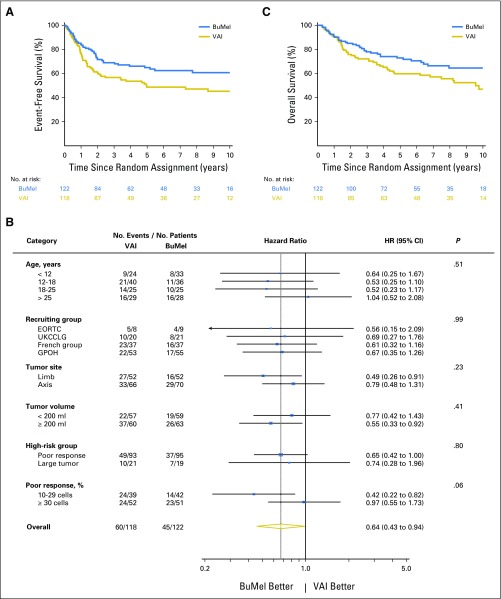
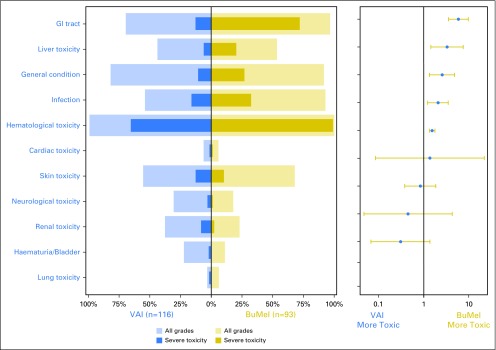
Purpose For over 30 years, the place of consolidation high-dose chemotherapy in Ewing sarcoma (ES) has been controversial. A randomized study was conducted to determine whether consolidation high-dose chemotherapy improved survival in patients with localized ES at high risk for relapse. Methods Randomization between busulfan and melphalan (BuMel) or standard chemotherapy (vincristine, dactinomycin, and ifosfamide [VAI], seven courses) was offered to patients if they were younger than 50 years of age with poor histologic response (≥ 10% viable cells) after receiving vincristine, ifosfamide, doxorubicin, and etoposide (six courses); or had a tumor volume at diagnosis ≥ 200 mL if unresected, or initially resected, or resected after radiotherapy. A 15% improvement in 3-year event-free survival (EFS) was sought (hazard ratio [HR], 0.60). Results Between 2000 and 2015, 240 patients classified as high risk (median age, 17.1 years) were randomly assigned to VAI (n = 118) or BuMel (n = 122). Seventy-eight percent entered the trial because of poor histologic response after chemotherapy alone. Median follow-up was 7.8 years. In an intent-to-treat analysis, the risk of event was significantly decreased by BuMel compared with VAI: HR, 0.64 (95% CI, 0.43 to 0.95; P = .026); 3- and 8-year EFS were, respectively, 69.0% (95% CI, 60.2% to 76.6%) versus 56.7% (95% CI, 47.6% to 65.4%) and 60.7% (95% CI, 51.1% to 69.6%) versus 47.1% (95% CI, 37.7% to 56.8%). Overall survival (OS) also favored BuMel: HR, 0.63 (95% CI, 0.41 to 0.95; P = .028); 3- and 8-year OS were, respectively, 78.0% (95% CI, 69.6% to 84.5%) versus 72.2% (95% CI, 63.3% to 79.6%) and 64.5% (95% CI, 54.4% to 73.5%) versus 55.6% (95% CI, 45.8% to 65.1%). Results were consistent in the sensitivity analysis. Two patients died as a result of BuMel-related toxicity, one after standard chemotherapy. Significantly more BuMel patients experienced severe acute toxicities from this course of chemotherapy compared with multiple VAI courses. Conclusion BuMel improved EFS and OS when given after vincristine, ifosfamide, doxorubicin, and etoposide induction in localized ES with predefined high-risk factors. For this group of patients, BuMel may be an important addition to the standard of care.
Figures
References
-
- Le Deley M-C, Paulussen M, Lewis I, et al. : Cyclophosphamide compared with ifosfamide in consolidation treatment of standard-risk Ewing sarcoma: Results of the randomized noninferiority Euro-EWING99-R1 trial. J Clin Oncol 32:2440-2448, 2014 - PubMed
-
- Paulussen M, Craft AW, Lewis I, et al. : Results of the EICESS-92 Study: Two randomized trials of Ewing’s sarcoma treatment--Cyclophosphamide compared with ifosfamide in standard-risk patients and assessment of benefit of etoposide added to standard treatment in high-risk patients. J Clin Oncol 26:4385-4393, 2008 - PubMed
-
- Bacci G, Forni C, Longhi A, et al: Long-term outcome for patients with non-metastatic Ewing’s sarcoma treated with adjuvant and neoadjuvant chemotherapies. 402 patients treated at Rizzoli between 1972 and 1992. Eur J Cancer40:73-83, 2004. - PubMed
-
- Cotterill SJ, Ahrens S, Paulussen M, et al. : Prognostic factors in Ewing’s tumor of bone: Analysis of 975 patients from the European Intergroup Cooperative Ewing’s Sarcoma Study Group. J Clin Oncol 18:3108-3114, 2000 - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
