

Mortality Changes Associated with Mandated Public Reporting for Sepsis. The Results of the New York State Initiative
- PMID: 30189749
- PMCID: PMC6290949
- DOI: 10.1164/rccm.201712-2545OC
Mortality Changes Associated with Mandated Public Reporting for Sepsis. The Results of the New York State Initiative
Abstract
Rationale: In 2013, the New York State Department of Health (NYSDOH) began a mandatory state-wide initiative to improve early recognition and treatment of severe sepsis and septic shock.
Objectives: This study examines protocol initiation, 3-hour and 6-hour sepsis bundle completion, and risk-adjusted hospital mortality among adult patients with severe sepsis and septic shock.
Methods: Cohort analysis included all patients from all 185 hospitals in New York State reported to the NYSDOH from April 1, 2014, to June 30, 2016. A total of 113,380 cases were submitted to NYSDOH, of which 91,357 hospitalizations from 183 hospitals met study inclusion criteria. NYSDOH required all hospitals to submit and follow evidence-informed protocols (including elements of 3-h and 6-h sepsis bundles: lactate measurement, early blood cultures and antibiotic administration, fluids, and vasopressors) for early identification and treatment of severe sepsis or septic shock.
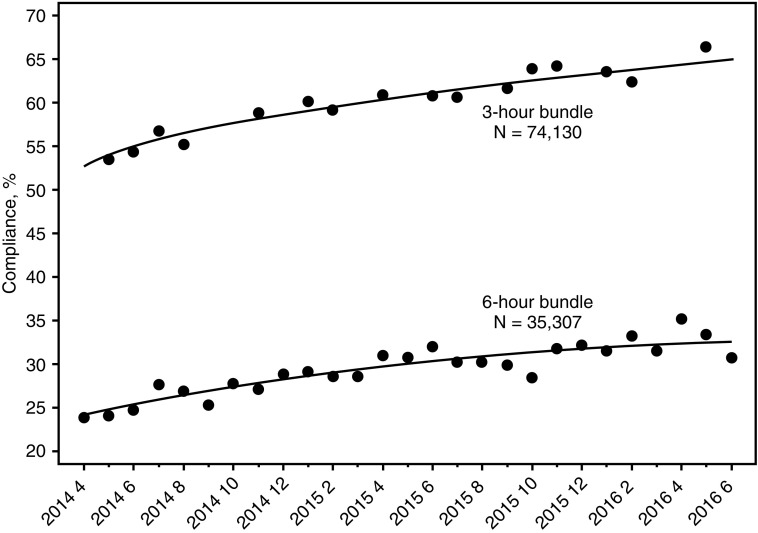
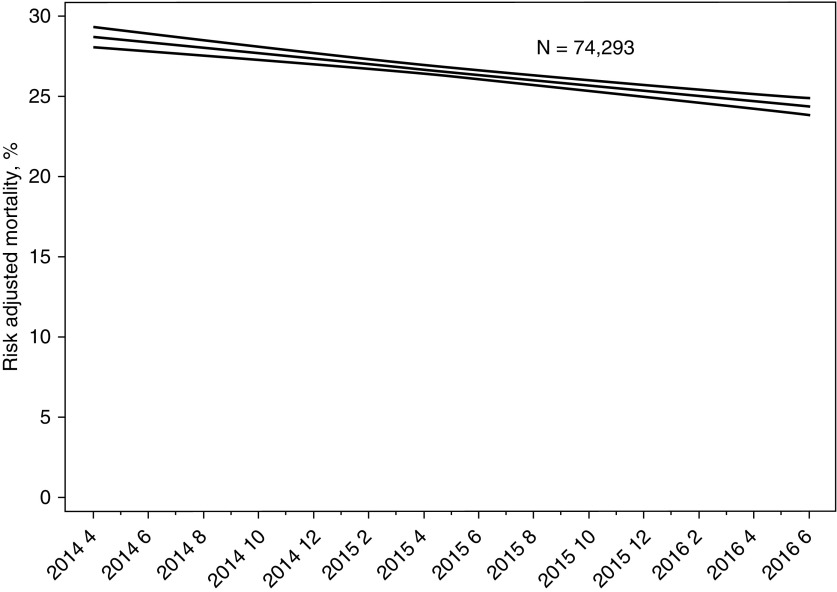
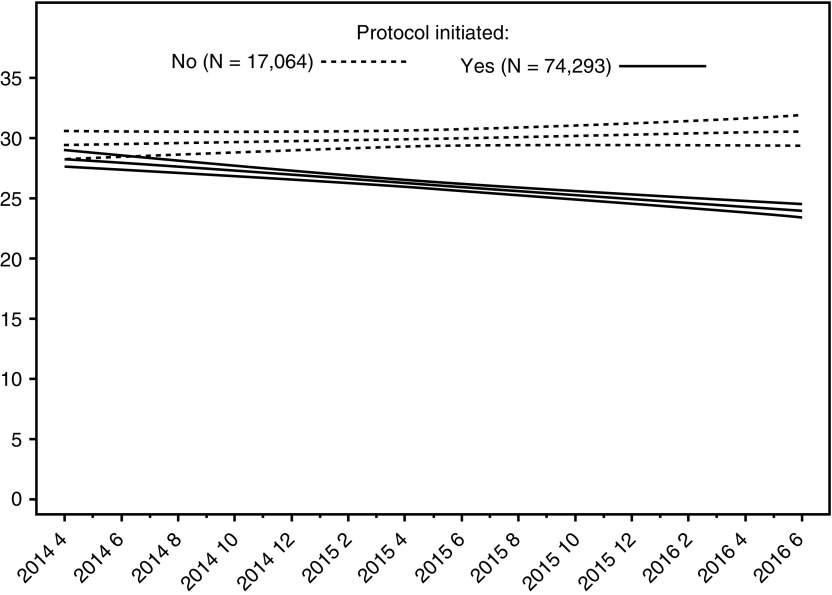
Measurements and main results: Compliance with elements of the sepsis bundles and risk-adjusted mortality were studied. Of 91,357 patients, 74,293 (81.3%) had the sepsis protocol initiated. Among these individuals, 3-hour bundle compliance increased from 53.4% to 64.7% during the study period (P < 0.001), whereas among those eligible for the 6-hour bundle (n = 35,307) compliance increased from 23.9% to 30.8% (P < 0.001). Risk-adjusted mortality decreased from 28.8% to 24.4% (P < 0.001) in patients among whom a sepsis protocol was initiated. Greater hospital compliance with 3-hour and 6-hour bundles was associated with shorter length of stay and lower risk and reliability-adjusted mortality.
Conclusions: New York's statewide initiative increased compliance with sepsis-performance measures. Risk-adjusted sepsis mortality decreased during the initiative and was associated with increased hospital-level compliance.
Keywords: implementation science; performance improvement; quality; sepsis.
Figures
Comment in
-
The Medical Perspective on a Disease Life Cycle. Sepsis in the Realm of Implementation Science.Am J Respir Crit Care Med. 2018 Dec 1;198(11):1360-1361. doi: 10.1164/rccm.201807-1293ED. Am J Respir Crit Care Med. 2018. PMID: 30230351 Free PMC article. No abstract available.
References
-
- Angus DC, Linde-Zwirble WT, Lidicker J, Clermont G, Carcillo J, Pinsky MR. Epidemiology of severe sepsis in the United States: analysis of incidence, outcome, and associated costs of care. Crit Care Med. 2001;29:1303–1310. - PubMed
-
- Martin GS, Mannino DM, Eaton S, Moss M. The epidemiology of sepsis in the United States from 1979 through 2000. N Engl J Med. 2003;348:1546–1554. - PubMed
-
- Elixhauser A, Friedman B, Stranges E. Septicemia in US Hospitals, HCUP Statistical Brief #122. Rockville, MD; 2011 [accessed 2011 Nov 18]. Available from: http://www.hcup-us.ahrq.gov/reports/statbriefs/sb122.pdf.
-
- Liu V, Escobar GJ, Greene JD, Soule J, Whippy A, Angus DC, et al. Hospital deaths in patients with sepsis from 2 independent cohorts. JAMA. 2014;312:90–92. - PubMed
-
- 10 CRR-NY 405.4. Westlaw. Thomson Reuters [accessed 2017 Feb 11]. Available from: https://govt.westlaw.com/nycrr/Document/I4fe39657cd1711dda432a117e6e0f34....
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
