

How has the cost of antiretroviral therapy changed over the years? A database analysis in Italy
- PMID: 30189882
- PMCID: PMC6127985
- DOI: 10.1186/s12913-018-3507-x
How has the cost of antiretroviral therapy changed over the years? A database analysis in Italy
Abstract
Background: The number of human immunodeficiency virus (HIV)-related hospitalizations has decreased worldwide in recent years, due to the availability of combined antiretroviral therapies (cART). The present analysis aimed to analyse the economic, and clinical burden of HIV management, after the introduction of systematic use of cART.
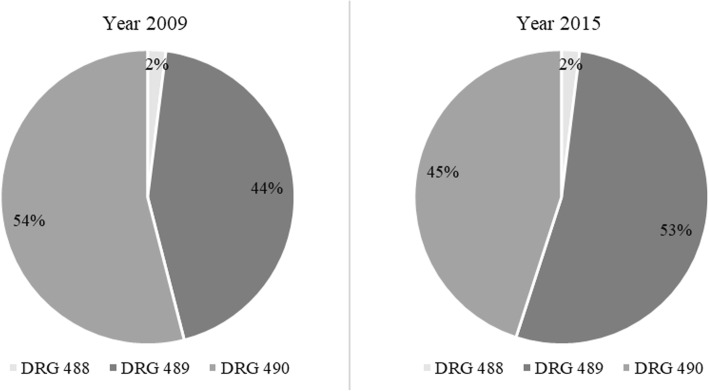
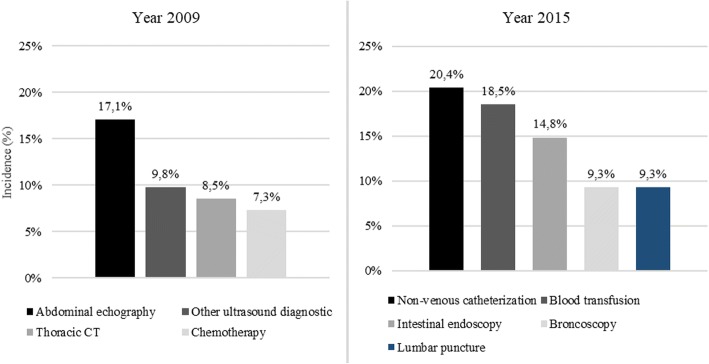
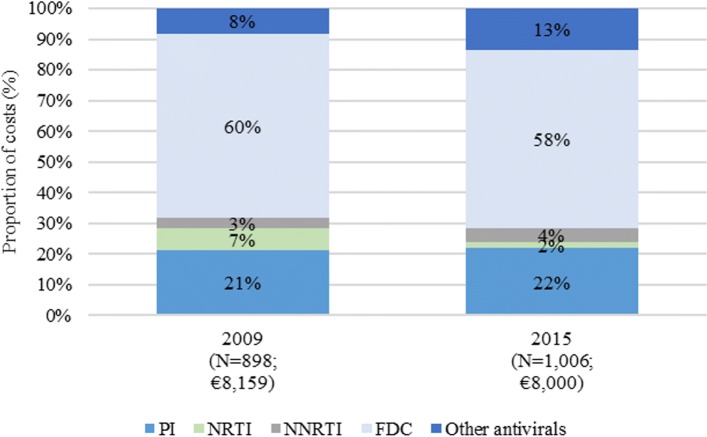
Methods: Data from HIV-infected patients, treated at Policlinico San Martino Hospital in Genova (Italy) were retrospectively collected. A comparison between years 2009 and 2015 was performed. HIV-related admissions were identified by using the Diagnosis-Related Group (DRG) codes. The resource consumption of outpatient services was derived by using a modelling approach. Expenditure for drugs was also analysed, as aggregate data.
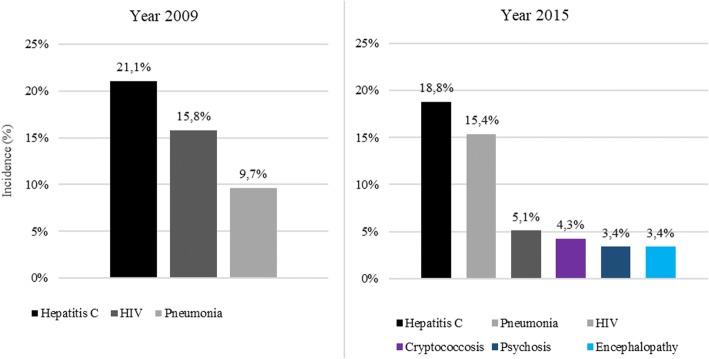
Results: The number of HIV-infected patients was 898 in 2009 and 1006 in 2015. Overall, the virological success rate improved from 2009 to 2015, as the percentage of patients with HIV-RNA < 50 copies/mL increased from 79 to 89% (P < 0.05). The average incidence of hospitalizations per-patient decreased from 0.30 in 2009, to 0.13 in 2015. Average expenditure per-patient decreased from €10,107 in 2009 to €9063 in 2015.
Conclusions: The present analysis confirmed the role of cART in controlling HIV viral load and, consequently, in reducing hospitalizations, admissions to day-hospital and the use of outpatient services. Clinical improvements and economic savings more than compensated the investments required to treat HIV-infected patients with cART. Health Authorities should invest in modern cART supply and universal treatment, to use at best the available resources and obtain a cost-effective improvement of health in people living with HIV. Additional research, with the involvement of different centers and the use of patient-specific data, are recommended to consolidate the findings of this analysis.
Keywords: AIDS; Antiretroviral; Burden; Cost; HIV; Hospitalization; cART.
Conflict of interest statement
Ethics approval and consent to participate
Ethics approvals were granted by the Ligurian Ethics Committee (approved on 28 August, 2013, 2/2013). Informed consent for the use of anonymized data for scientific purposes was signed by all patients admitted to Hospital and included in the study.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- UNAIDS . Fact sheet - latest global and regional statistics on the status of the AIDS epidemic. 2017. GLOBAL HIV STATISTICS.
-
- UNAIDS. HIV and AIDS estimates in Italy, 2016. http://www.unaids.org/en/regionscountries/countries/italy. Accessed 6 June 2018.
-
- Quiros-Roldan E, Magoni M, Raffetti E, et al. The burden of chronic diseases and cost-of-care in subjects with HIV infection in a Health District of northern Italy over a 12-year period compared to that of the general population. BMC Public Health. 2016;16:1146. doi: 10.1186/s12889-016-3804-4. - DOI - PMC - PubMed
-
- Torti C, Casari S, Palvarini L, et al. Modifications of health resource-use in Italy after the introduction of highly active antiretroviral therapy (HAART) for human immunodeficiency virus (HIV) infection. Pharmaco-economic implications in a population-based setting. Health Policy. 2003;65(3):261–267. doi: 10.1016/S0168-8510(03)00002-2. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
