

Spanish Lymphoma Group (GELTAMO) guidelines for the diagnosis, staging, treatment, and follow-up of diffuse large B-cell lymphoma
- PMID: 30190794
- PMCID: PMC6122355
- DOI: 10.18632/oncotarget.25892
Spanish Lymphoma Group (GELTAMO) guidelines for the diagnosis, staging, treatment, and follow-up of diffuse large B-cell lymphoma
Abstract
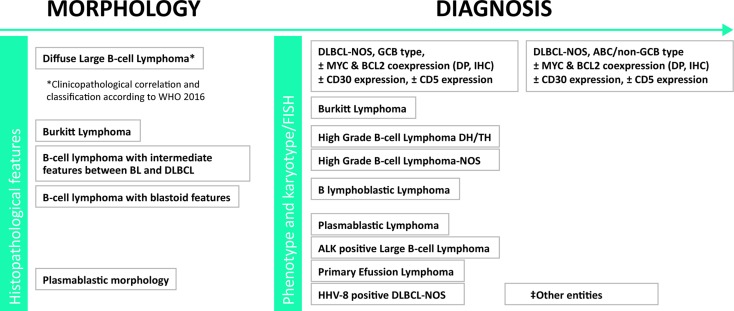
Diffuse large B-cell lymphoma (DLBCL) accounts for approximately 30% of non-Hodgkin lymphoma (NHL) cases in adult series. DLBCL is characterized by marked clinical and biological heterogeneity, encompassing up to 16 distinct clinicopathological entities. While current treatments are effective in 60% to 70% of patients, those who are resistant to treatment continue to die from this disease. An expert panel performed a systematic review of all data on the diagnosis, prognosis, and treatment of DLBCL published in PubMed, EMBASE and MEDLINE up to December 2017. Recommendations were classified in accordance with the Grading of Recommendations Assessment Development and Evaluation (GRADE) framework, and the proposed recommendations incorporated into practical algorithms. Initial discussions between experts began in March 2016, and a final consensus was reached in November 2017. The final document was reviewed by all authors in February 2018 and by the Scientific Committee of the Spanish Lymphoma Group GELTAMO.
Keywords: DLBCL; DLBCL entities; guidelines; risk assessment; treatment.
Conflict of interest statement
CONFLICTS OF INTEREST EGB has received honoraria as speaker from Roche and has served as a consultant to and received compensation from Servier, Sanofi, Gilead, and Janssen. MC declares that she has no relevant or material financial interests that relate to the research described in this paper. AM has received honoraria as a speaker from Celgene, Janssen, Roche, and Servier, honoraria for participating in advisory boards from Gilead, Celgene, Servier, and Roche, and research support from Janssen. CM has received honoraria as a speaker from Takeda. SMM has served as a consultant to and has received compensation from Roche and Takeda. CP has received honoraria as a speaker from Takeda, Janssen, and Roche and has served as a consultant to and received compensation from Servier, Takeda, and Janssen. GR has received honoraria as a speaker from Roche, Takeda, Janssen, Celgene, and Servier and has received honoraria for participation in advisory boards from Janssen, Celgene, and BMS. JMS has received honoraria as a speaker from Roche, Gilead, Celgene, Janssen, and Mundipharma, honoraria for participation in advisory boards from Roche, Gilead, Janssen, Sanofi, and Servier, and research support from Teva. AL has received honoraria as a speaker from Servier, Janssen, Gilead, Celgene, and Takeda, honoraria for participation in advisory boards from Gilead, Takeda, and Servier, and research support from Roche. There are no other potential conflicts of interest relevant to this paper to be declared.
Figures
References
-
- Montes-Moreno S, Mollejo Villanueva M, Fraga M, García JF, Villar JL, Martínez A, Rodríguez Pinilla SM, Battle A, Pulla MP, Rozman M, García Sanz R. Recomendaciones para el estudio histopatológico, inmunohistoquímico, citogenético y molecular e informe diagnóstico de los procesos neoplásicos linfoides. Consenso SEAP-SEHH-GOTEL. En: Libro Blanco de la Anatomía Patológica en España. 2017. pp. 63–174. Available at: https://www.seap.es/libros-blancos.
-
- Alizadeh AA, Eisen MB, Davis RE, Ma C, Lossos IS, Rosenwald A, Boldrick JC, Sabet H, Tran T, Yu X, Powell JI, Yang L, Marti GE, et al. Distinct types of diffuse large B-cell lymphoma identified by gene expression profiling. Nature. 2000;403:503–11. - PubMed
-
- Hans CP, Weisenburger DD, Greiner TC, Gascoyne RD, Delabie J, Ott G, Müller-Hermelink HK, Campo E, Braziel RM, Jaffe ES, Pan Z, Farinha P, Smith LM, et al. Confirmation of the molecular classification of diffuse large B-cell lymphoma by immunohistochemistry using a tissue microarray. Blood. 2004;103:275–82. - PubMed
-
- Choi WW, Weisenburger DD, Greiner TC, Piris MA, Banham AH, Delabie J, Braziel RM, Geng H, Iqbal J, Lenz G, Vose JM, Hans CP, Fu K, et al. A New Immunostain Algorithm Classifies Diffuse Large B-Cell Lymphoma into Molecular Subtypes with High Accuracy. Clin Cancer Res. 2009;15:5494–502. - PMC - PubMed
-
- Johnson NA, Slack GW, Savage KJ, Connors JM, Ben-Neriah S, Rogic S, Scott DW, Tan KL, Steidl C, Sehn LH, Chan WC, Iqbal J, Meyer PN, et al. Concurrent Expression of MYC and BCL2 in Diffuse Large B-Cell Lymphoma Treated With Rituximab Plus Cyclophosphamide, Doxorubicin, Vincristine, and Prednisone. J Clin Oncol. 2012;30:3452–9. - PMC - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
