

Melanoma and nuclear medicine
- PMID: 30190811
- PMCID: PMC6094667
- DOI: 10.2217/mmt.14.10
Melanoma and nuclear medicine
Abstract
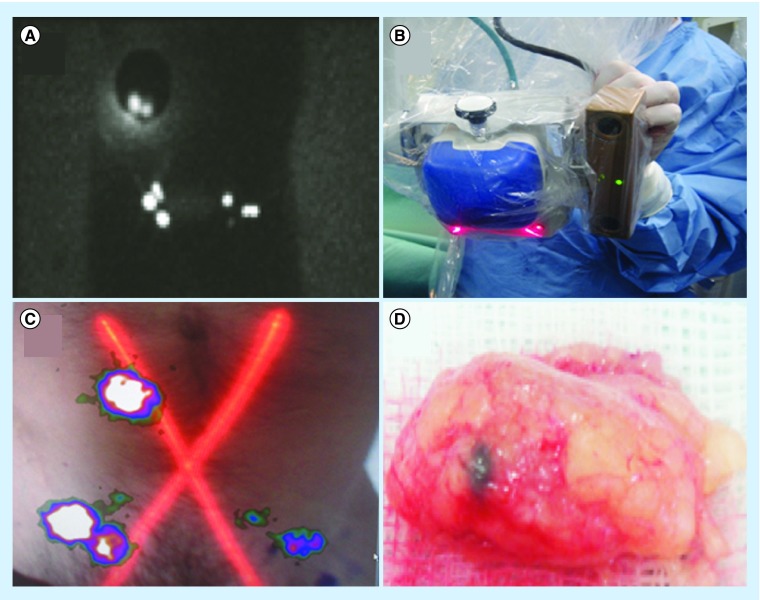
Supported by a large body of published work, the contribution of nuclear medicine technologies to the assessment of melanoma has been increasing in recent years. Lymphoscintigraphy-assisted sentinel lymph node biopsy and PET are in continuous evolution with the aid of technological imaging advances, making it possible to fuse functional and anatomic images (e.g., with SPECT/CT, PET/CT and 3D rendering systems). The development of hybrid fluorescent-radioactive tracers that enable high-quality preoperative lymphoscintigraphy and SPECT/CT, and the optimization of modern intraoperative portable imaging technologies, such as free-hand SPECT and portable γ-cameras, are important innovations that have improved sentinel lymph node identification in complex anatomical areas, such as the pelvis and head and neck. Concurrently, 18F-fluorodeoxyglucose-PET has proved its usefulness in the clinical staging and treatment decision-making process, and there is also emerging evidence regarding its utility in the evaluation of therapeutic response. The potential uses of other novel PET radiotracers could open up a new field of use for this technique. In this article, we review the current and future role of nuclear medicine in the management of melanoma.
Keywords: PET/CT; fluorescence; lymph node biopsy; melanoma; portable imaging technologies; radio-guided surgery.
Conflict of interest statement
Financial & competing interests disclosure The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. No writing assistance was utilized in the production of this manuscript.
Figures






References
-
- WHO Ultraviolet radiation and the INTERSUN Programme. http://www.who.int/uv/faq/skincancer/en/index1.html
-
- Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J. Clin. Oncol. 2001;19(16):3622–3634. - PubMed
-
- Testori A, De Salvo GL, Montesco MC, et al. Clinical considerations on sentinel node biopsy in melanoma from an Italian multicentric study on 1,313 patients (SOLISM-IMI) Ann. Surg. Oncol. 2009;16(7):2018–2027. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources