

PD-L1 in melanoma: facts and myths
- PMID: 30190888
- PMCID: PMC6096437
- DOI: 10.2217/mmt-2016-0013
PD-L1 in melanoma: facts and myths
Abstract
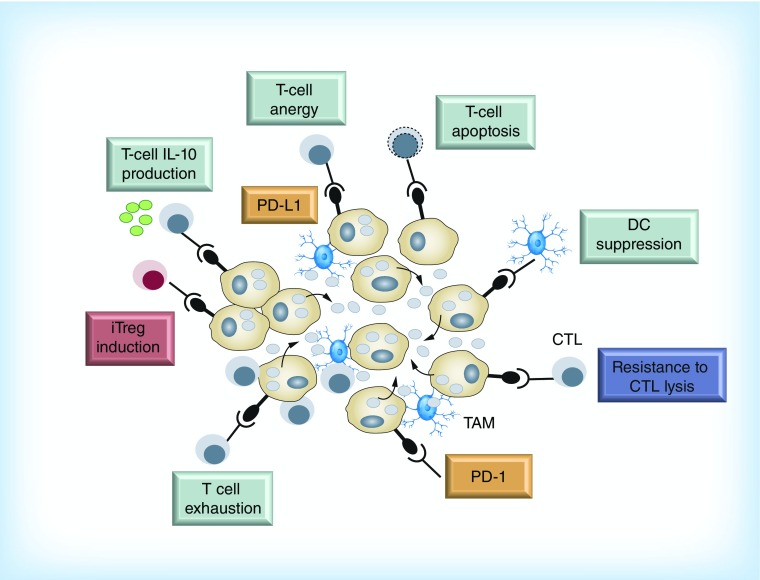
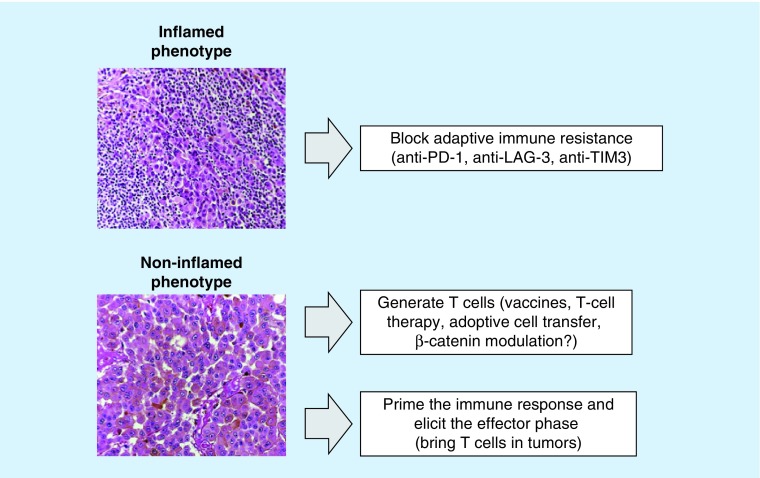
The use of monoclonal antibodies that block immunologic checkpoints that would otherwise mediate the adaptive immune resistance have paved the way in cancer treatment. There is evidence that blocking the PD-1/PD-L1 axis is a strategy of overriding importance in the treatment of patients with metastatic melanoma and other solid malignancies, some of which (NSCLC, colorectal cancer, renal cell cancer, head and neck cancer) were not considered to be 'immune-responsive' diseases until recently. In this perspective article, the biological and clinical relevance of PD-L1 is summarized in the context of the immune checkpoint inhibitors as a therapeutic strategy in metastatic melanoma patients.
Keywords: PD-1; PD-L1; immune checkpoint inhibitors; melanoma; predictive; prognostic.
Conflict of interest statement
Financial & competing interests disclosure The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. No writing assistance was utilized in the production of this manuscript.
Figures
References
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials