

Melanoma & nuclear medicine: new insights & advances
- PMID: 30190932
- PMCID: PMC6122522
- DOI: 10.2217/mmt-2017-0022
Melanoma & nuclear medicine: new insights & advances
Abstract
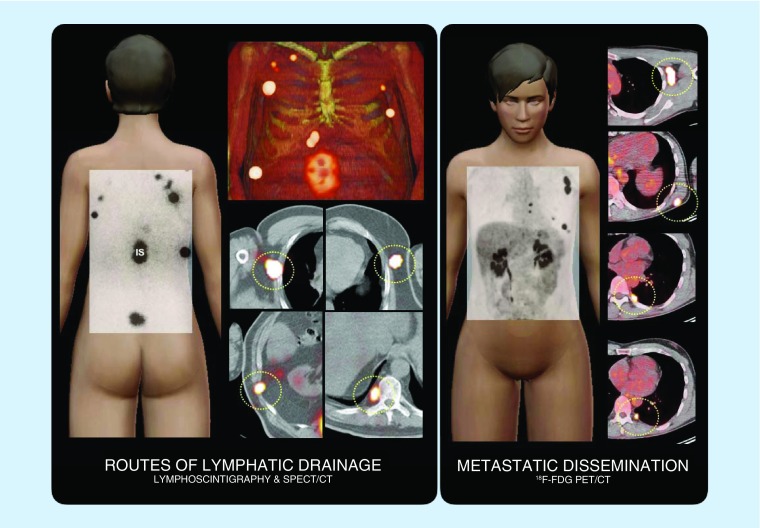
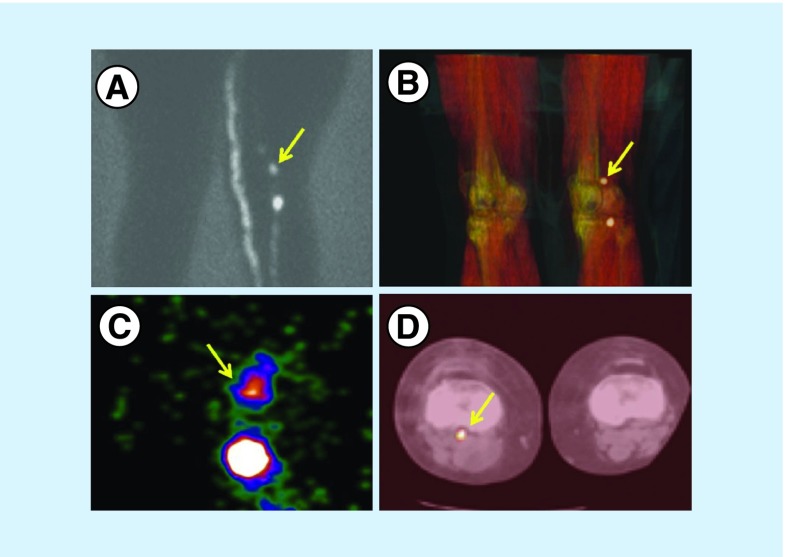
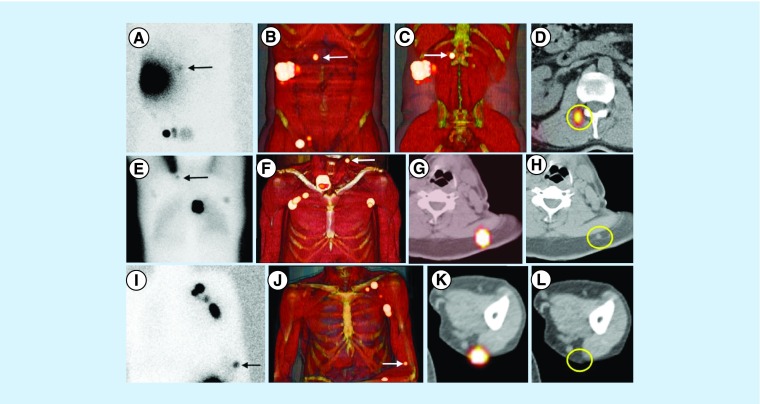
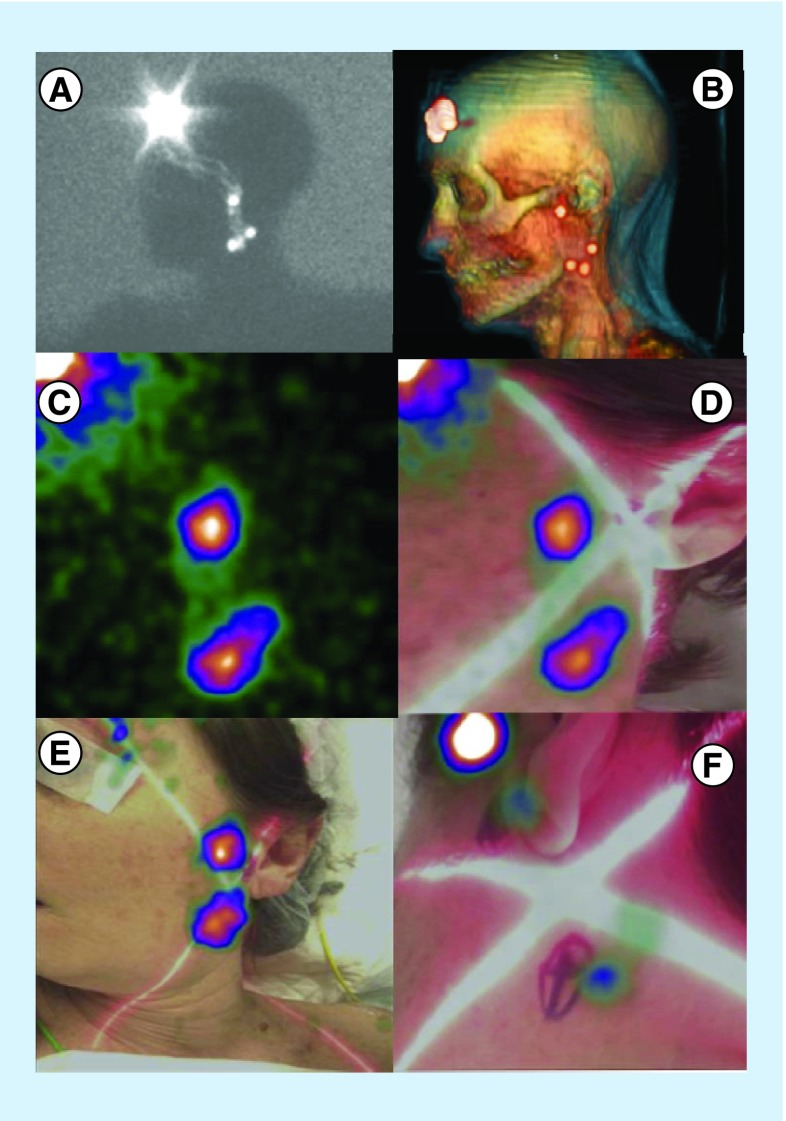
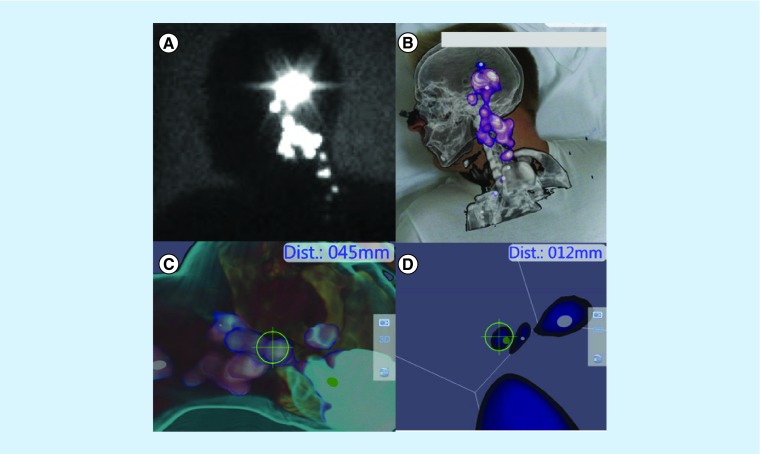
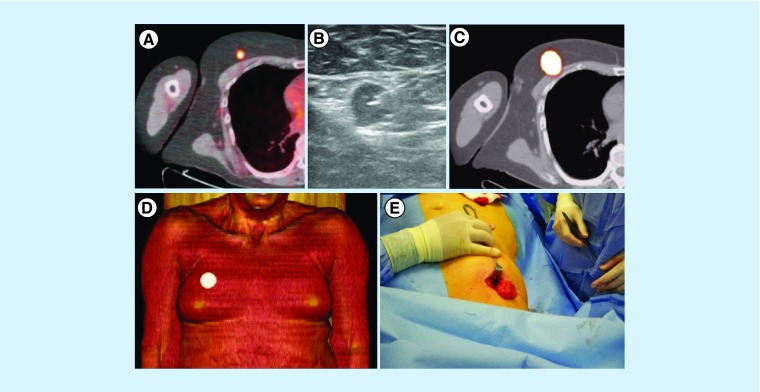
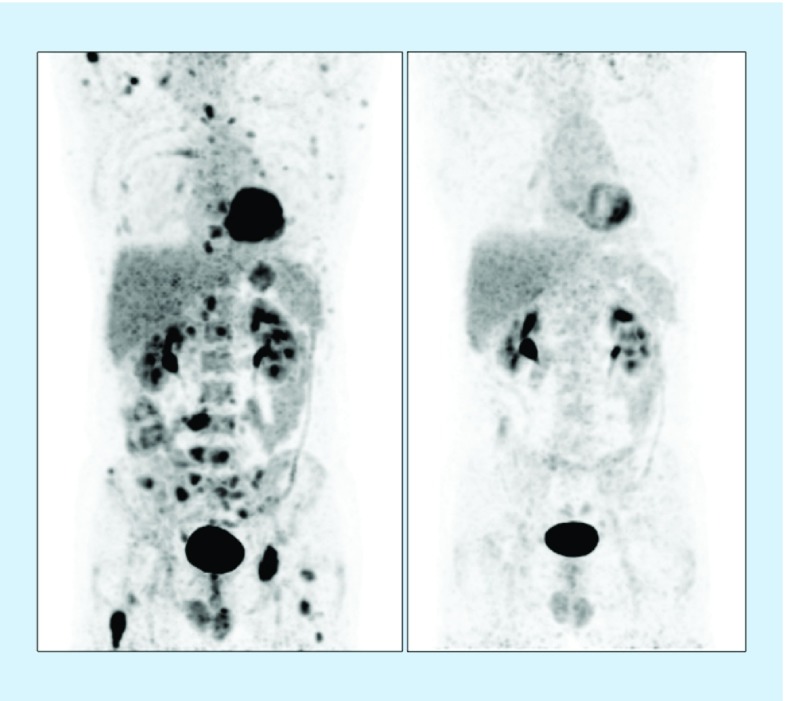
The contribution of nuclear medicine to management of melanoma patients is increasing. In intermediate-thickness N0 melanomas, lymphoscintigraphy provides a roadmap for sentinel node biopsy. With the introduction of single-photon emission computed tomography images with integrated computed tomography (SPECT/CT), 3D anatomic environments for accurate surgical planning are now possible. Sentinel node identification in intricate anatomical areas (pelvic cavity, head/neck) has been improved using hybrid radioactive/fluorescent tracers, preoperative lymphoscintigraphy and SPECT/CT together with modern intraoperative portable imaging technologies for surgical navigation (free-hand SPECT, portable gamma cameras). Furthermore, PET/CT today provides 3D roadmaps to resect 18F-fluorodeoxyglucose-avid melanoma lesions. Simultaneously, in advanced-stage melanoma and recurrences, 18F-fluorodeoxyglucose-PET/CT is useful in clinical staging and treatment decision as well as in the evaluation of therapy response. In this article, we review new insights and recent nuclear medicine advances in the management of melanoma patients.
Keywords: 18F-FDG-PET/CT; SPECT/CT; intraoperative technologies; radioguided surgery; sentinel node biopsy.
Conflict of interest statement
Financial & competing interests disclosure The authors have no relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript. This includes employment, consultancies, honoraria, stock ownership or options, expert testimony, grants or patents received or pending, or royalties. No writing assistance was utilized in the production of this manuscript.
Figures


References
-
- Balch CM, Soong SJ, Gershenwald JE, et al. Prognostic factors analysis of 17,600 melanoma patients: validation of the American Joint Committee on Cancer melanoma staging system. J. Clin. Oncol. 2001;19(16):3622–3634. - PubMed
-
- Morton DL, Cochran AJ, Thompson JF, et al. Sentinel node biopsy for early-stage melanoma: accuracy and morbidity in MSLT-I, an international multicenter trial. Ann. Surg. 2005;242(3):302–311. - PMC - PubMed
-
•• Prospective multicenter study that confirmed the value of early nodal evaluation and treatment of melanoma based on sentinel node biopsy (SNB).
-
- Morton DL, Thompson JF, Cochran AJ, et al. Sentinel-node biopsy or nodal observation in melanoma. N. Engl. J. Med. 2006;355(13):1307–1317. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources