

Surgical treatment of hepatocellular carcinoma: should resection be performed according to Barcelona Clinic Liver Cancer classification?
- PMID: 30191006
- PMCID: PMC6095418
- DOI: 10.2217/hep.15.18
Surgical treatment of hepatocellular carcinoma: should resection be performed according to Barcelona Clinic Liver Cancer classification?
Abstract
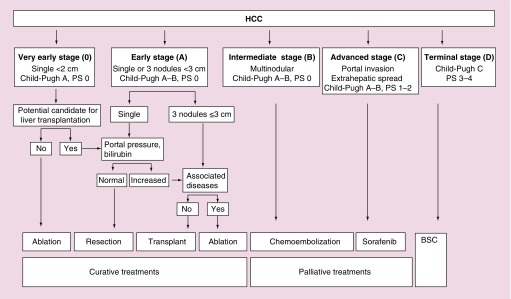
The best results in surgical resection are obtained in patients with solitary tumors without clinically significant portal hypertension (hepatic venous pressure gradient >10 mmHg). In such settings, 5-year survival rates exceed 70%. When portal hypertension exceeds this cut-off value, 5-year survival decreases to 55%, as is also the case in patients with more than one nodule. Surgery may be technically feasible, in other words, with acceptable 30-day mortalities although the clinically relevant survival outcome is significantly reduced. In such instances, patients may be better served by liver transplantation. If this option is not available, the outcome may not differ to that obtained by ablation for small solitary hepatocellular carcinoma or for chemoembolization for those patients with multifocal hepatocellular carcinoma within the Milan criteria. This philosophy is the backbone for the Barcelona Clinic Liver Cancer decision-making process.
Keywords: BCLC classification; HVPG; Milan criteria; expanded criteria; hepatocellular carcinoma; liver resection; liver transplantation; portal hypertension; vascular invasion.
Conflict of interest statement
Financial & competing interests disclosure J Fuster has been funded by an investigation grant from Association Llavaneres contra el Cáncer. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- Llovet JM, Bruix J, Gores G. Surgical resection vs transplantation for early hepatocellular carcinoma: clues for the best strategy. Hepatology. 2000;31:1919–1921. - PubMed
-
- Poon RT, Fan ST. Hepatectomy for hepatocellular carcinoma: patient selection and postoperative outcome. Liver. Transplant. 2004;(Suppl. 1):S39–S45. - PubMed
-
- Bruix J, Sherman M. Management of hepatocellular carcinoma. Hepatology. 2005;42:519–524. - PubMed
-
•• A practice guidelines on the management of hepatocellular carcinoma published by the American Association for the Study of Liver Diseases (AASLD).
-
- Llovet JM, Fuster J, Bruix J. Intention to treat analysis of surgical treatment for early hepatocellular carcinoma: resection vs transplantation. Hepatology. 1999;39:1434–1440. - PubMed
-
•• After listing for orthotopic liver transplantation, patients have to wait for a variable period of time during which the tumor may progress and preclude the operation. This adverse event worsens the outcomes when an intention-to-treat analysis of orthotopic liver transplantation results is performed.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources