

Management of metastatic melanoma: improved survival in a national cohort following the approvals of checkpoint blockade immunotherapies and targeted therapies
- PMID: 30191256
- PMCID: PMC6249064
- DOI: 10.1007/s00262-018-2241-x
Management of metastatic melanoma: improved survival in a national cohort following the approvals of checkpoint blockade immunotherapies and targeted therapies
Abstract
Background: Immune checkpoint blockade (ICB) and BRAFV600-targeted therapy have demonstrated substantial clinical efficacy for patients with stage 4 melanoma in clinical trials; however, their impact on survival and barriers to treatment in the "real-life" setting remains unknown.
Methods: Patients who presented with cutaneous melanoma during 2004-2015 using the National Cancer Database, which comprises > 70% of all newly diagnosed cancers in the U.S., were evaluated for predictors of presenting with stage 4 disease and receiving ICB, and for their associated unadjusted and risk-adjusted overall survival (OS).
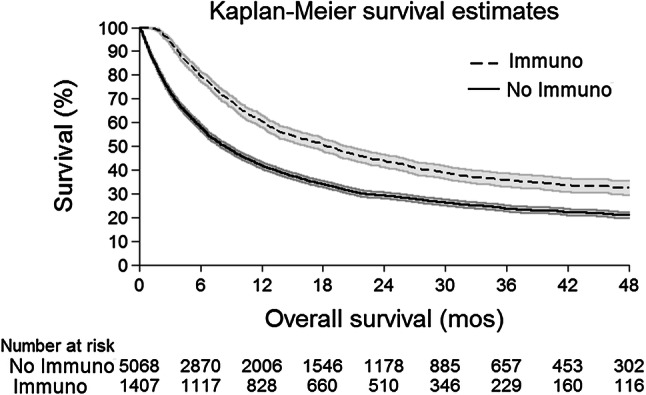
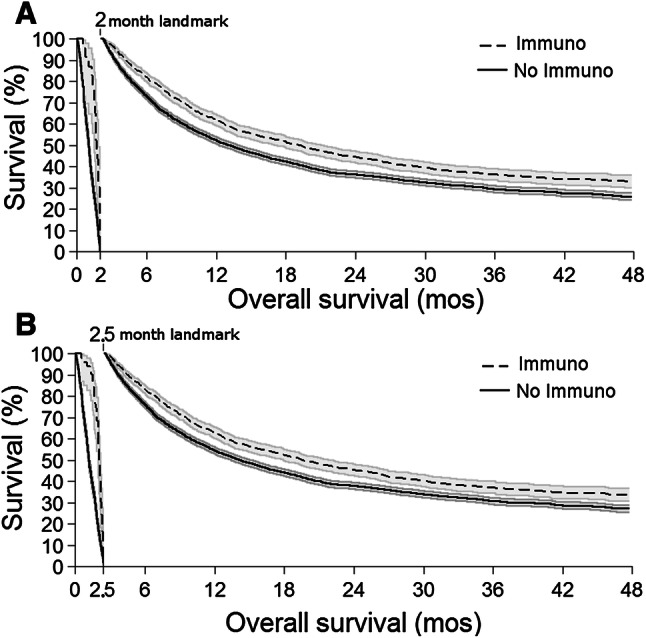
Results: 17,975 patients presented with stage 4 metastatic cutaneous melanoma. Overall, patients who presented after the FDA's initial approvals (starting in 2011) for ICB and BRAFV600-targeted therapy demonstrated a 31% relative improvement in 4-year OS (p < 0.001), compared to pre-2011. Following the initial approvals in 2011, improved OS was associated in risk-adjusted analyses with ICB (HR 0.57, 95CI 0.52-0.63). ICB demonstrated improved median and 4-year OS of 16.9 months (95CI 15.6-19.3; vs. 7.7 months, 95CI 7.2-8.4) and 32.4% (95CI 29.5-35.3; vs. 21.0%, 95CI 19.6-22.2, all p < 0.001), respectively; improved OS was persistent in unadjusted and risk-adjusted landmark survival analyses. Uninsured patients and management in the community setting were less likely to receive ICB in multivariable analyses.
Conclusions: In a national "real-life" treatment population, we show that the wide availability of the novel treatment modalities ICB and BRAFV600-targeted therapy has significantly improved the survival of patients with stage 4 melanoma. Our findings additionally suggest that there are opportunities for expanding coverage and access to these novel immunotherapies in community practice.
Keywords: Immune checkpoint blockade; Immunotherapy; Melanoma; Metastasis; Targeted therapy.
Conflict of interest statement
The authors declare that they have no conflicts of interest.
Figures
References
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
