

Aortic remodeling with frozen elephant trunk technique for Stanford type A aortic dissection using Japanese J-graft open stent graft
- PMID: 30191318
- PMCID: PMC6510868
- DOI: 10.1007/s00380-018-1246-x
Aortic remodeling with frozen elephant trunk technique for Stanford type A aortic dissection using Japanese J-graft open stent graft
Erratum in
-
Correction to: Aortic remodeling with frozen elephant trunk technique for Stanford type A aortic dissection using Japanese J-graft open stent graft.Heart Vessels. 2019 Feb;34(2):316-317. doi: 10.1007/s00380-018-1268-4. Heart Vessels. 2019. PMID: 30259173 Free PMC article.
Abstract
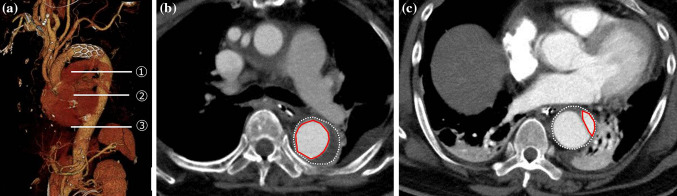
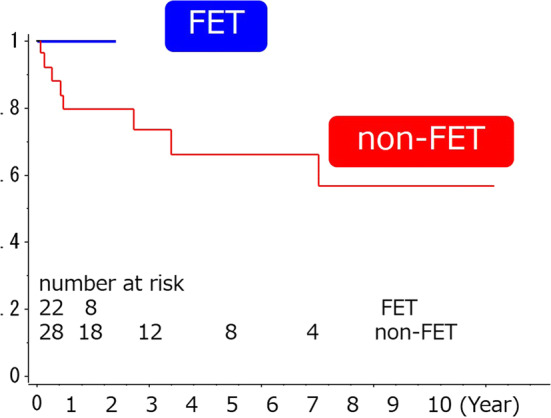
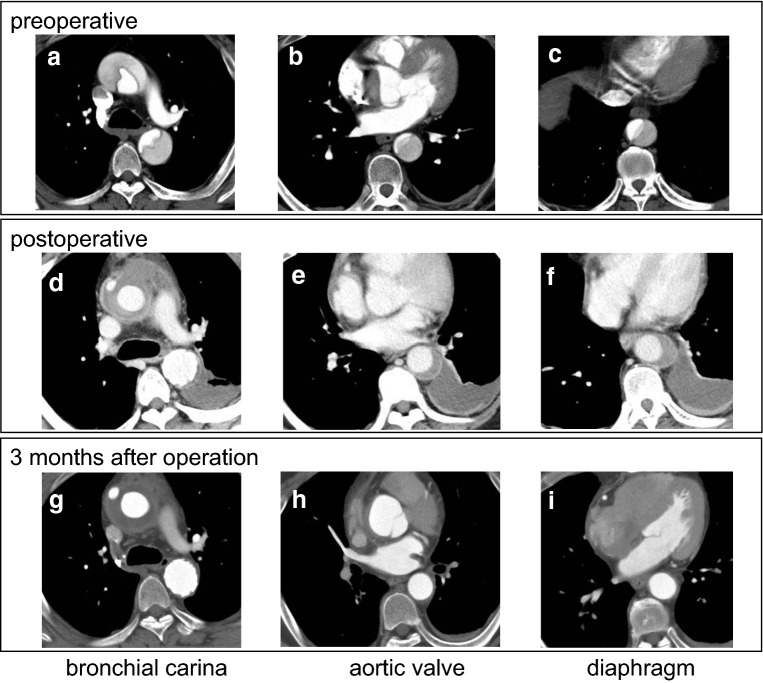
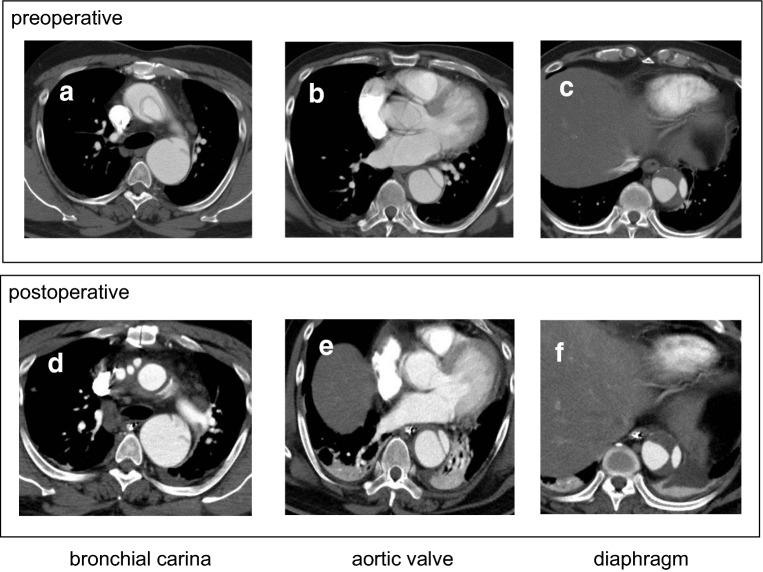
The frozen elephant trunk (FET) technique allows single-stage extended surgical repair of Stanford type A aortic dissection and has shown promotion of aortic remodeling by maintaining the true lumen flow and facilitating its expansion and by promoting false lumen thrombosis. However, few studies have compared the effectiveness of FET technique, in terms of the downstream aortic remodeling. Between 2005 and 2017, 50 patients underwent total arch replacement for Stanford type A aortic dissection, including that with (n = 22) and without FET technique (n = 28). We compared distal aortic remodeling in patients who underwent total arch replacement with (using a J-Graft open stent graft) or without the technique. The false lumen complete thrombosis rate and the ratio of true lumen area at three levels of the descending aorta were evaluated post operation. In FET group, the diameter and length of the stent graft were 29.0 ± 3.9 mm and 70.9 ± 17.4 mm, respectively. The in-hospital death with and without the FET technique was 0 and 3, respectively, with no late death in both groups. Eight patients (28.6%) only in the non-FET group required additional surgical treatment for downstream aorta. In the FET group, the ratio of true lumen area at the level of bronchial carina and false lumen complete thrombosis rate at the levels of bronchial carina and aortic valve were significantly higher than non-FET group. A more favorable remodeling in the descending aorta was observed in patients who underwent FET associated with a total arch replacement compared to those who underwent total arch replacement alone.
Keywords: Aortic dissection; Aortic remodeling; Frozen elephant trunk.
Conflict of interest statement
All the authors have declared no competing interest.
Figures
References
-
- Committee for Scientific Affairs TJAfTS. Masuda M, Okumura M, Doki Y, Endo S, Hirata Y, Kobayashi J, Kuwano H, Motomura N, Nishida H, Saiki Y, Saito A, Shimizu H, Tanaka F, Tanemoto K, Toh Y, Tsukihara H, Wakui S, Yokomise H. Thoracic and cardiovascular surgery in Japan during 2014: annual report by The Japanese Association for Thoracic Surgery. Gen Thorac Cardiovasc Surg. 2016;64:665–697. doi: 10.1007/s11748-016-0695-3. - DOI - PMC - PubMed
-
- Castrovinci S, Pacini D, Di Marco L, Berretta P, Cefarelli M, Murana G, Alfonsi J, Pantaleo A, Leone A, Di Eusanio M, Di Bartolomeo R. Surgical management of aortic root in type A acute aortic dissection: a propensity-score analysis. Eur J Cardiothorac Surg. 2016;50:223–229. doi: 10.1093/ejcts/ezw038. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
