

Functional and educational outcomes after treatment for intracranial arteriovenous malformations in children
- PMID: 30191363
- PMCID: PMC6209013
- DOI: 10.1007/s00701-018-3665-y
Functional and educational outcomes after treatment for intracranial arteriovenous malformations in children
Abstract
Background: Arteriovenous malformations (AVMs) in the pediatric population are rare, yet they form the most frequent cause of hemorrhagic stroke in children. Compared to adults, children have been suggested to have beneficial neurological outcomes. However, few studies have focused on other variables than neurological outcomes. This study aims to assess the long-term functional and educational outcomes of children after multimodality approach of treatment for intracranial AVMs.
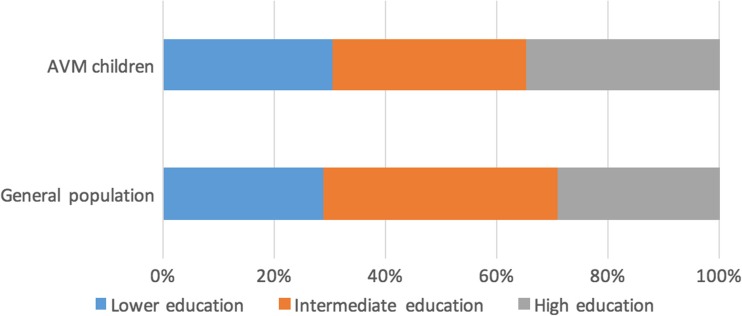
Methods: All children treated in our center between 1998 and 2016 for intracranial AVMs were reviewed. Patient characteristics, as well as AVM specifics, were collected. Functional outcomes were compared using the modified Rankin scale (mRs). Educational levels, using the International Standard Classification of Education (ISCED), were compared to the age-matched general population of the Netherlands.
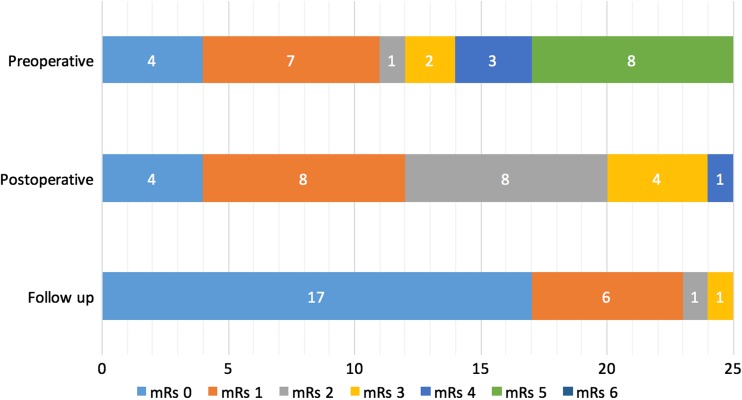
Results: In total, 25 children were included at mean age of 10 years (range 2-16 years). Nineteen patients (76%) presented with intracranial bleeding. Mean follow-up was 11.5 ± 5.3 years (range 4.1-24.4). Four (16%) of patients were treated with embolization, three (12%) with microsurgery, and 18 patients (72%) received a combination of different treatment modalities. Altogether, 21 (84%) were embolized, 14 (56%) were treated with microsurgery, and eight (32%) received stereotactic radiosurgery. One child had a worse mRs at discharge compared to admission; all others improved (n = 11) or were stable (n = 13). At follow-up, all patients scored a stable or improved mRs compared to discharge, with 23 children (92%) scoring mRs 0 or 1. These 23 children followed regular education during follow-up without specialized or adapted schooling. No significant differences in educational level with the age-matched general population were found.
Conclusion: This retrospective review shows positive long-term results of both functional and educational outcomes after multidisciplinary treatment of pediatric brain AVMs.
Keywords: Arteriovenous malformation; Development; Education; Functional outcomes; Multimodality treatment; Pediatrics.
Conflict of interest statement
Conflict of interest
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements) or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
Ethical approval
This article does not contain any studies with human participants performed by any of the authors. Our institutional ethical board exempted this study, due to the retrospective nature, from the requirement of formal consent.
Figures
References
-
- Abecassis IJ, Nerva JD, Barber J, Rockhill J, Ellenbogen RG, Kim LJ, Sekhar LN. Toward a comprehensive assessment of functional outcomes in pediatric patients with brain arteriovenous malformations: the Pediatric Quality of Life Inventory. J Neurosurg Pediatr. 2016;18(5):611–622. doi: 10.3171/2016.6.PEDS16103. - DOI - PubMed
-
- Blauwblomme T, Bourgeois M, Meyer P, Puget S, Di Rocco F, Boddaert N, Zerah M, Brunelle F, Sainte RC, Naggara O. Long-term outcome of 106 consecutive pediatric ruptured brain arteriovenous malformations after combined treatment. Stroke. 2014;45(6):1664–1671. doi: 10.1161/STROKEAHA.113.004292. - DOI - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
