

Hospital-acquired colonization and infections in a Vietnamese intensive care unit
- PMID: 30192894
- PMCID: PMC6128614
- DOI: 10.1371/journal.pone.0203600
Hospital-acquired colonization and infections in a Vietnamese intensive care unit
Abstract
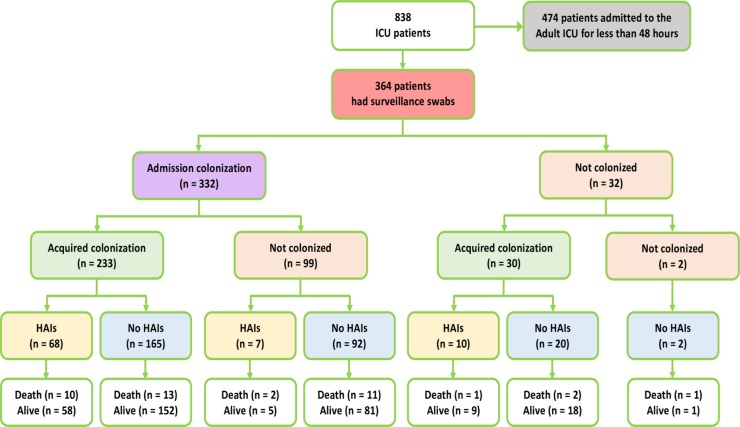
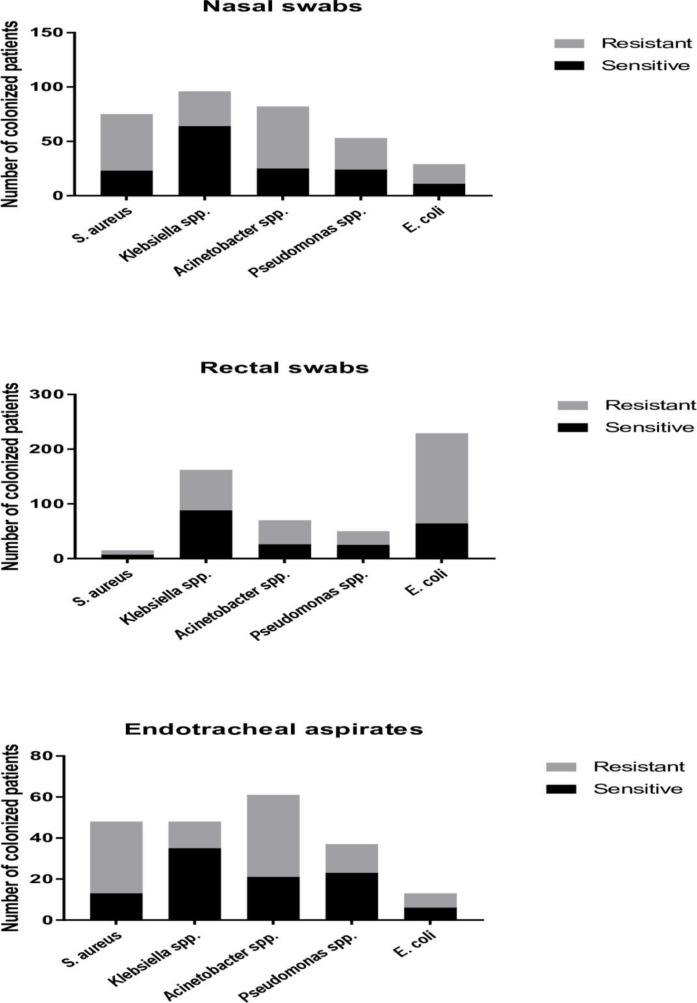
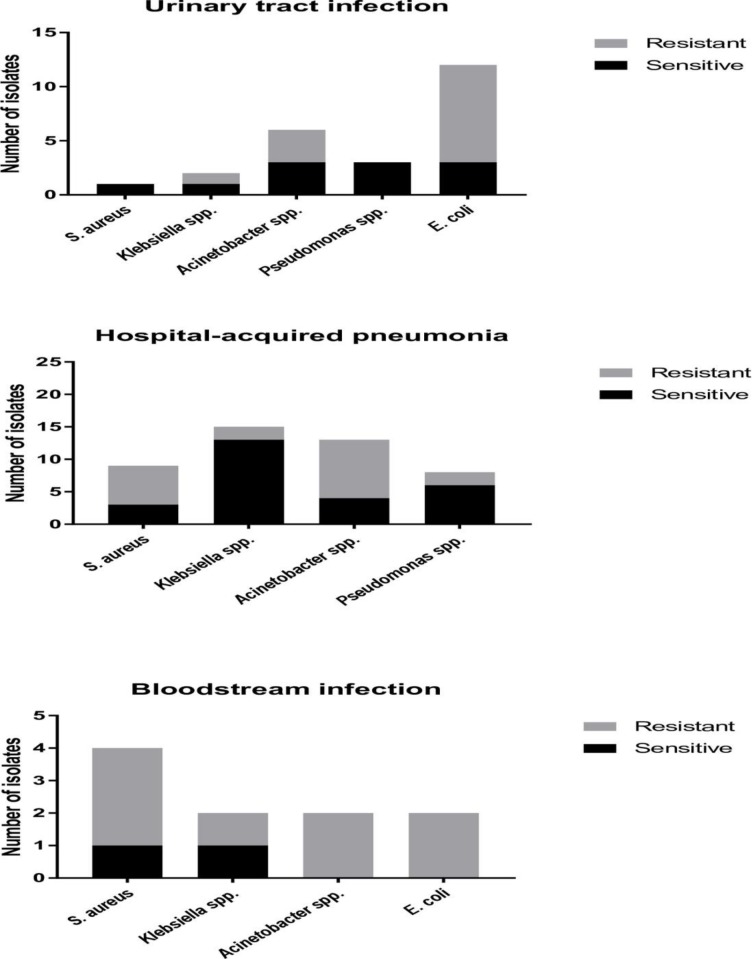
Data concerning intensive care unit (ICU)-acquired bacterial colonization and infections are scarce from low and middle-income countries (LMICs). ICU patients in these settings are at high risk of becoming colonized and infected with antimicrobial-resistant organisms (AROs). We conducted a prospective observational study at the Ho Chi Minh City Hospital for Tropical Diseases, Vietnam from November 2014 to January 2016 to assess the ICU-acquired colonization and infections, focusing on the five major pathogens in our setting: Staphylococcus aureus (S. aureus), Escherichia coli (E. coli), Klebsiella spp., Pseudomonas spp. and Acinetobacter spp., among adult patients with more than 48 hours of ICU stay. We found that 61.3% (223/364) of ICU patients became colonized with AROs: 44.2% (161/364) with rectal ESBL-producing E. coli and Klebsiella spp.; 30.8% (40/130) with endotracheal carbapenemase-producing Acinetobacter spp.; and 14.3% (52/364) with nasal methicillin-resistant S. aureus. The incidence rate of ICU patients becoming colonized with AROs was 9.8 (223/2,276) per 100 patient days. Significant risk factor for AROs colonization was the Charlson Comorbidity Index score. The proportion of ICU patients with HAIs was 23.4% (85/364), and the incidence rate of ICU patients contracting HAIs was 2.3 (85/3,701) per 100 patient days. The vascular catheterization (central venous, arterial and hemofiltration catheter) was significantly associated with hospital-acquired bloodstream infection. Of the 77 patients who developed ICU-acquired infections with one of the five specified bacteria, 44 (57.1%) had prior colonization with the same organism. Vietnamese ICU patients have a high colonization rate with AROs and a high risk of subsequent infections. Future research should focus on monitoring colonization and the development of preventive measures that may halt spread of AROs in ICU settings.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
References
-
- World Health Organization. Report on the Burden of Endemic Health Care-Associated Infection Worldwide. 2011;40.
-
- Ewans TM, Ortiz CR LF. Prevention and control of nosocomial infection in the intensive care unit Intensive Care Med 4th ed Lippincot-Raven, New York: 1999;1074–80.
-
- Elston J, Hinitt I, Batson S, Noakes C, Wright J, Walley J, et al. Infection control in a developing world. 2013;67(10):45–50. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
