

Frailty in the End-Stage Lung Disease or Heart Failure Patient: Implications for the Perioperative Transplant Clinician
- PMID: 30193783
- PMCID: PMC6368901
- DOI: 10.1053/j.jvca.2018.08.002
Frailty in the End-Stage Lung Disease or Heart Failure Patient: Implications for the Perioperative Transplant Clinician
Abstract
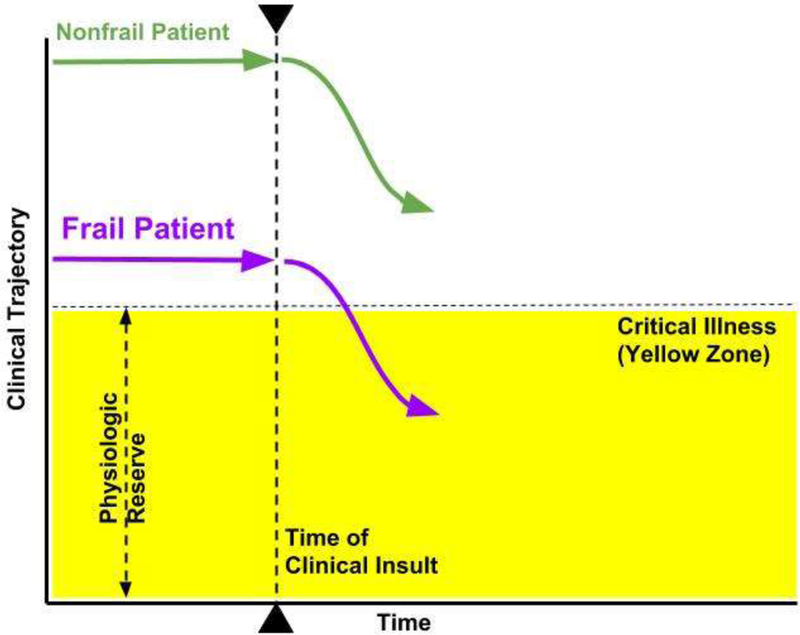
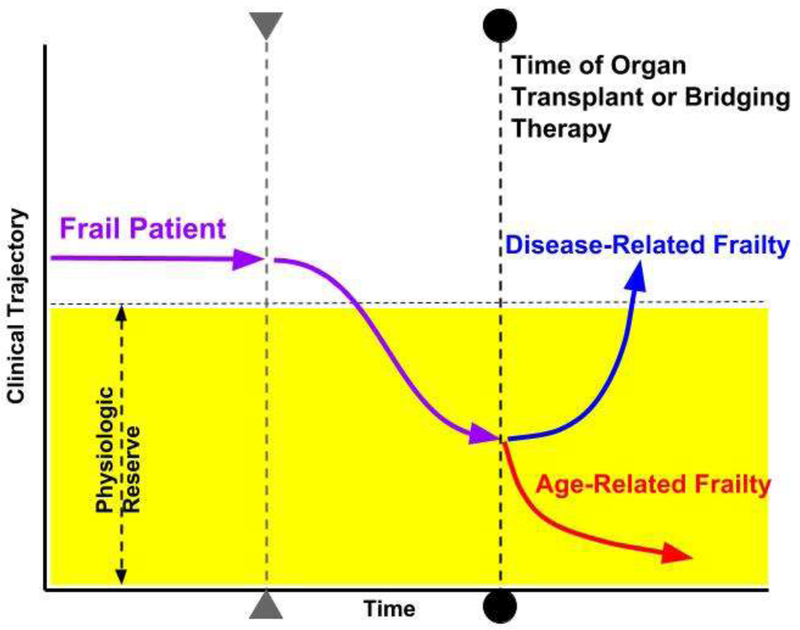
The syndrome of frailty for patients undergoing heart or lung transplantation has been a recent focus for perioperative clinicians because of its association with postoperative complications and poor outcomes. Patients with end-stage cardiac or pulmonary failure may be under consideration for heart or lung transplantation along with bridging therapies such as ventricular assist device implantation or venovenous extracorporeal membrane oxygenation, respectively. Early identification of frail patients in an attempt to modify the risk of postoperative morbidity and mortality has become an important area of study over the last decade. Many quantification tools and risk prediction models for frailty have been developed but have not been evaluated extensively or standardized in the cardiothoracic transplant candidate population. Heightened awareness of frailty, coupled with a better understanding of distinct cellular mechanisms and biomarkers apart from end-stage organ disease, may play an important role in potentially reversing frailty related to organ failure. Furthermore, the clinical management of these critically ill patients may be enhanced by waitlist and postoperative physical rehabilitation and nutritional optimization.
Keywords: COPD; ECMO; IABP; ICU; IGF-1; LVAD; biomarker; cachexia; cardiothoracic surgery; chronic lung disease; critical care; frailty; growth hormone; heart failure; heart transplantation; lung transplantation; metabolism; nutrition; rehabilitation; sarcopenia.
Copyright © 2018 Elsevier Inc. All rights reserved.
Figures
References
-
- Quarterly Data Report [ https://www.ishlt.org/registries/quarterlyDataReport.asp]
-
- Sepehri A, Beggs T, Hassan A et al. The impact of frailty on outcomes after cardiac surgery: a systematic review. J Thorac Cardiovasc Surg 2014; 148:3110–7. - PubMed
-
- Furukawa H, Tanemoto K. Frailty in cardiothoracic surgery: systematic review of the literature. Gen Thorac Cardiovasc Surg 2015; 63:425–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
