

Risk factors for mortality after respiratory syncytial virus lower respiratory tract infection in adults with hematologic malignancies
- PMID: 30195271
- PMCID: PMC6329612
- DOI: 10.1111/tid.12994
Risk factors for mortality after respiratory syncytial virus lower respiratory tract infection in adults with hematologic malignancies
Abstract
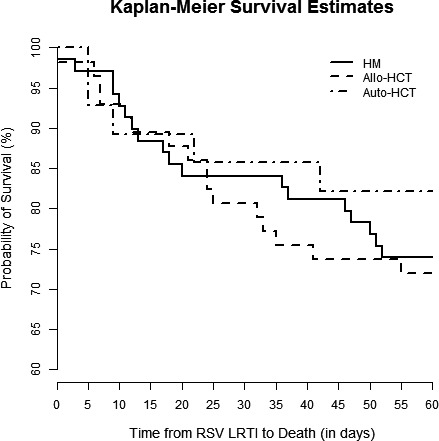
Background: Respiratory syncytial virus (RSV) lower respiratory tract infection (LRTI) is associated with high mortality in patients with hematologic malignancies (HM). We sought to determine whether allogeneic hematopoietic cell transplant (allo-HCT) recipients would be at higher risk for 60-day mortality.
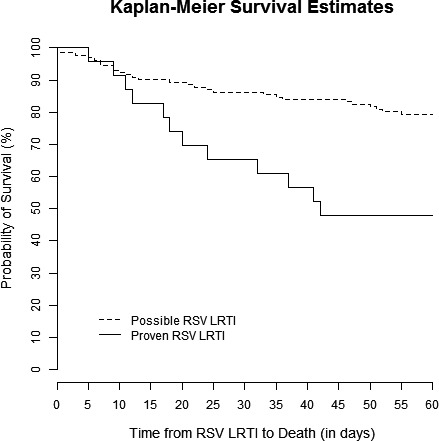
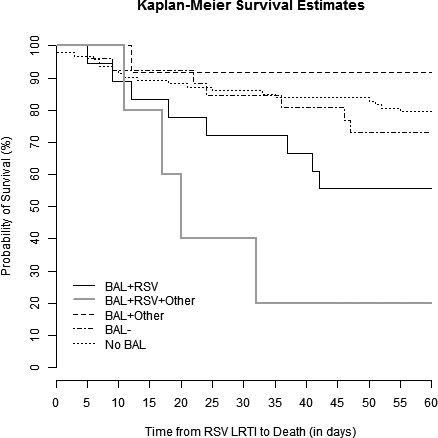
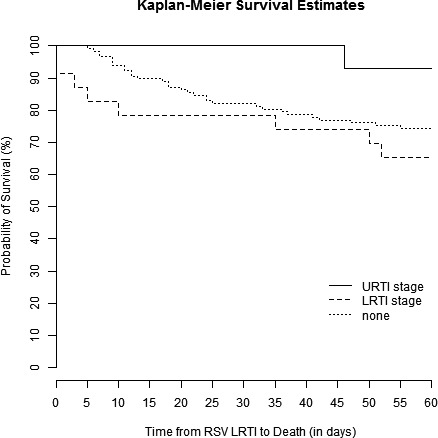
Methods: We examined a retrospective cohort of adults with HM with or without HCT treated for RSV LRTI (n = 154) at our institution from 1996-2013. We defined possible RSV LRTI as RSV detected only in the upper respiratory tract with new radiologic infiltrates and proven RSV LRTI as RSV detected in BAL fluid with new radiologic infiltrates. Immunodeficiency Scoring Index (ISI) and Severe Immunodeficiency (SID) criteria were calculated for HCT recipients. Multivariable logistic regression analyses were performed to identify independent risk factors associated with 60-day all-cause mortality.
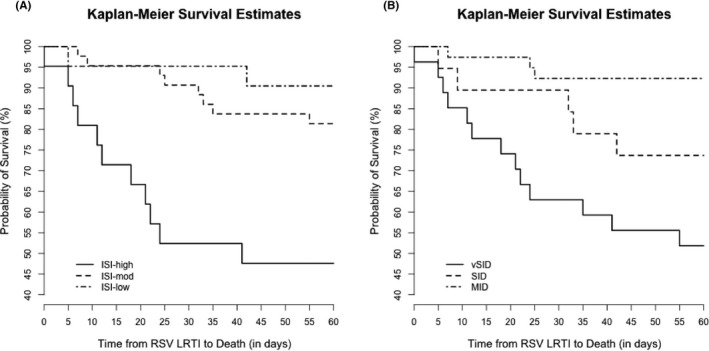
Results: Mortality was high in HM patients (25%), but there was no difference between those without HCT, autologous or allo-HCT recipients in logistic regression models. Separate multivariate models showed that at RSV diagnosis, neutropenia (OR 8.3, 95% CI 2.8-24.2, P = 0.005) and lymphopenia (OR 3.7, 95% CI 1.7-8.2, P = 0.001) were associated with 60-day mortality. Proven LRTI was associated with higher 60-day mortality (neutropenia model: OR 4.7, 95%CI 1.7-13.5; lymphopenia model: OR 3.3, 95% CI 1.2-8.8), and higher ICU admission. In HCT recipients, high ISI and very severe immunodeficiency by SID criteria were associated with higher 60-day all-cause mortality.
Conclusions: Mortality is similarly high among HM patients without HCT and HCT recipients. High-grade immunodeficiency and detection of RSV from BAL fluid are associated with higher 60-day mortality.
Keywords: hematologic malignancy; hematopoietic cell transplantation; lower respiratory tract infection; mortality; respiratory syncytial virus.
© 2018 John Wiley & Sons A/S. Published by John Wiley & Sons Ltd.
Conflict of interest statement
RFC receives research grants from Gilead and Consulting/Advisory Boards honoraria from Ablynx, Janssen, and ADMA Biologics. All other authors report no potential conflicts of interest.
Figures
References
-
- Falsey AR, Hennessey PA, Formica MA, Cox C, Walsh EE. Respiratory syncytial virus infection in elderly and high‐risk adults. N Engl J Med. 2005;352:1749‐1759. - PubMed
-
- Shah JN, Chemaly RF. Management of RSV infections in adult recipients of hematopoietic stem cell transplantation. Blood. 2011;117:2755‐2763. - PubMed
-
- Bowden RA. Respiratory virus infections after marrow transplant: the Fred Hutchinson Cancer Research Center experience. Am J Med. 1997;102:27‐30. - PubMed
-
- Ljungman P, Ward KN, Crooks BN, et al. Respiratory virus infections after stem cell transplantation: a prospective study from the Infectious Diseases Working Party of the European Group for Blood and Marrow Transplantation. Bone Marrow Transplant. 2001;28:479‐484. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
