

Neonatal cerebrovascular autoregulation
- PMID: 30196311
- PMCID: PMC6422675
- DOI: 10.1038/s41390-018-0141-6
Neonatal cerebrovascular autoregulation
Abstract
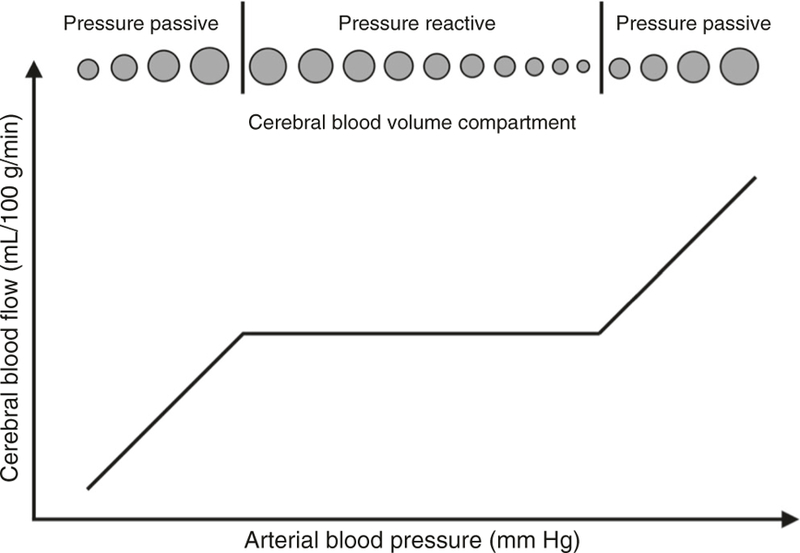
Cerebrovascular pressure autoregulation is the physiologic mechanism that holds cerebral blood flow (CBF) relatively constant across changes in cerebral perfusion pressure (CPP). Cerebral vasoreactivity refers to the vasoconstriction and vasodilation that occur during fluctuations in arterial blood pressure (ABP) to maintain autoregulation. These are vital protective mechanisms of the brain. Impairments in pressure autoregulation increase the risk of brain injury and persistent neurologic disability. Autoregulation may be impaired during various neonatal disease states including prematurity, hypoxic-ischemic encephalopathy (HIE), intraventricular hemorrhage, congenital cardiac disease, and infants requiring extracorporeal membrane oxygenation (ECMO). Because infants are exquisitely sensitive to changes in cerebral blood flow (CBF), both hypoperfusion and hyperperfusion can cause significant neurologic injury. We will review neonatal pressure autoregulation and autoregulation monitoring techniques with a focus on brain protection. Current clinical therapies have failed to fully prevent permanent brain injuries in neonates. Adjuvant treatments that support and optimize autoregulation may improve neurologic outcomes.
Figures
References
-
- Helou S, Koehler RC, Gleason CA, Jones MD & Traystman RJ Cerebrovascular autoregulation during fetal development in sheep. Am. J. Physiol. Heart C 266, H1069–H1074 (1994). - PubMed
-
- Rorke LB Anatomical features of the developing brain implicated in pathogenesis of hypoxic-ischemic injury. Brain. Pathol 2, 211–221 (1992). - PubMed
-
- Wladimiroff JW & van Bel F Fetal and neonatal cerebral blood flow. Semin. Perinatol 11, 335–346 (1987). - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
