

Heterogeneous distribution of trastuzumab in HER2-positive xenografts and metastases: role of the tumor microenvironment
- PMID: 30196384
- PMCID: PMC6209006
- DOI: 10.1007/s10585-018-9929-3
Heterogeneous distribution of trastuzumab in HER2-positive xenografts and metastases: role of the tumor microenvironment
Abstract
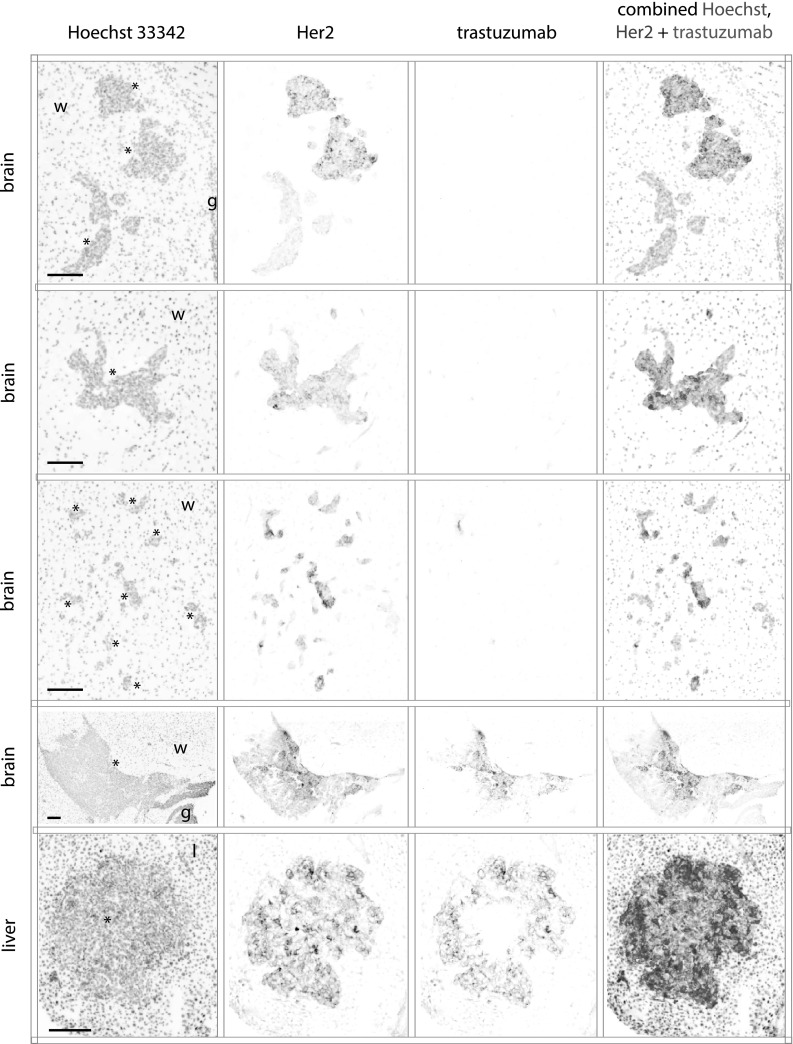
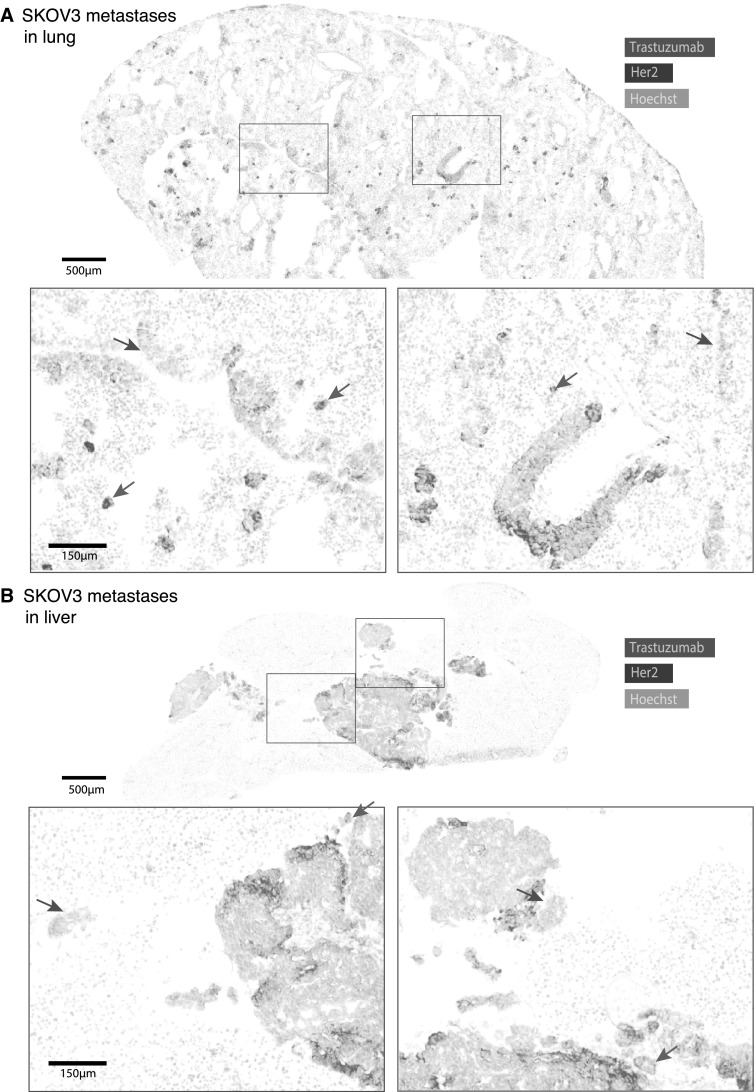
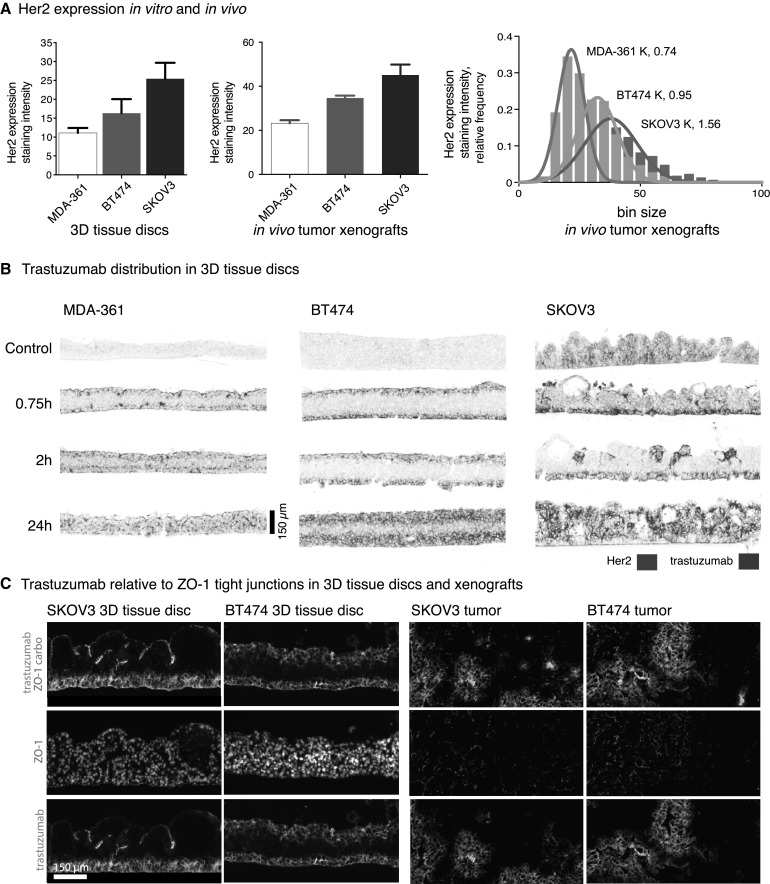
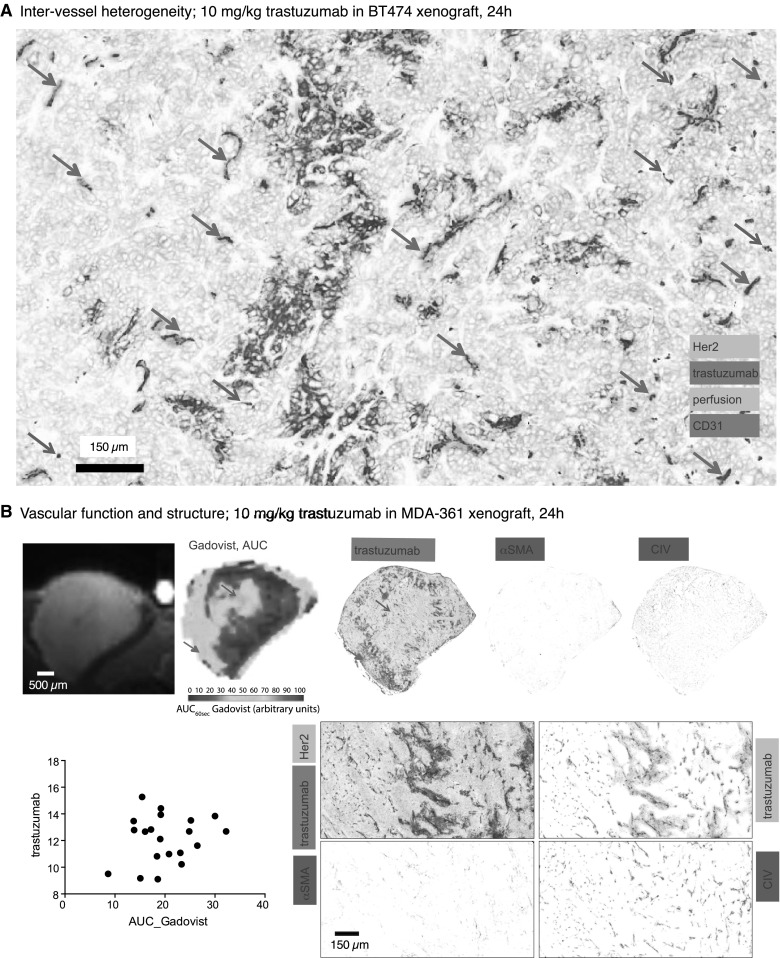
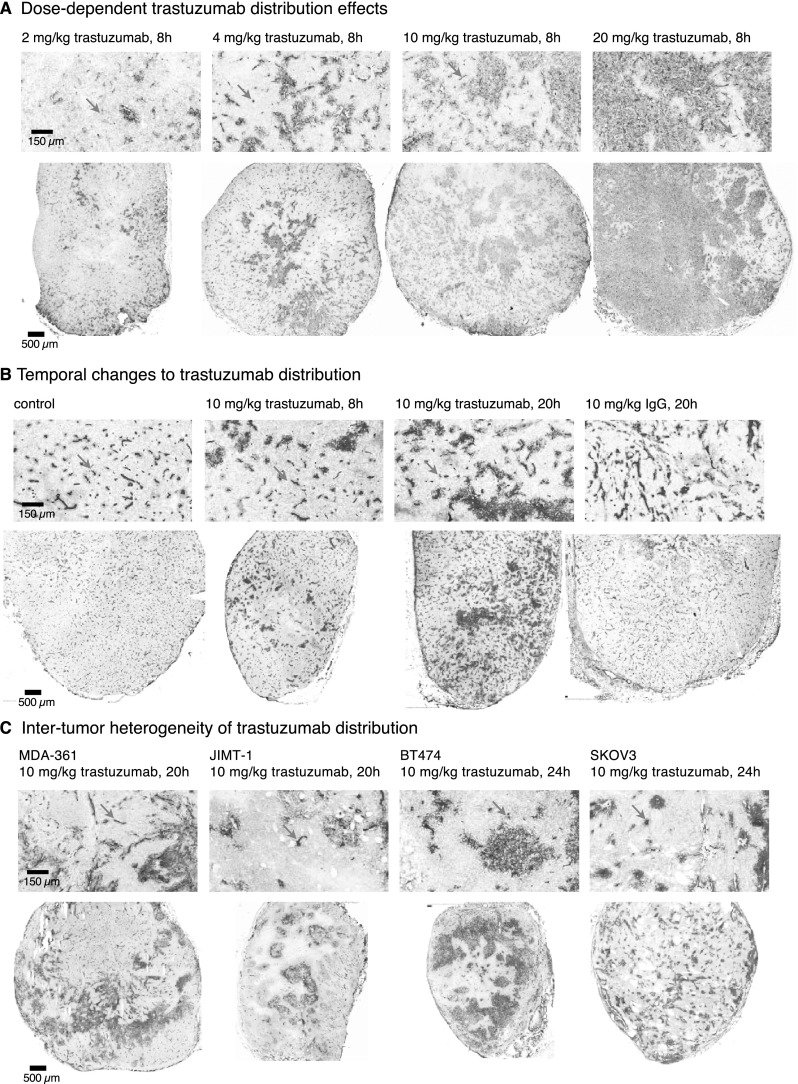
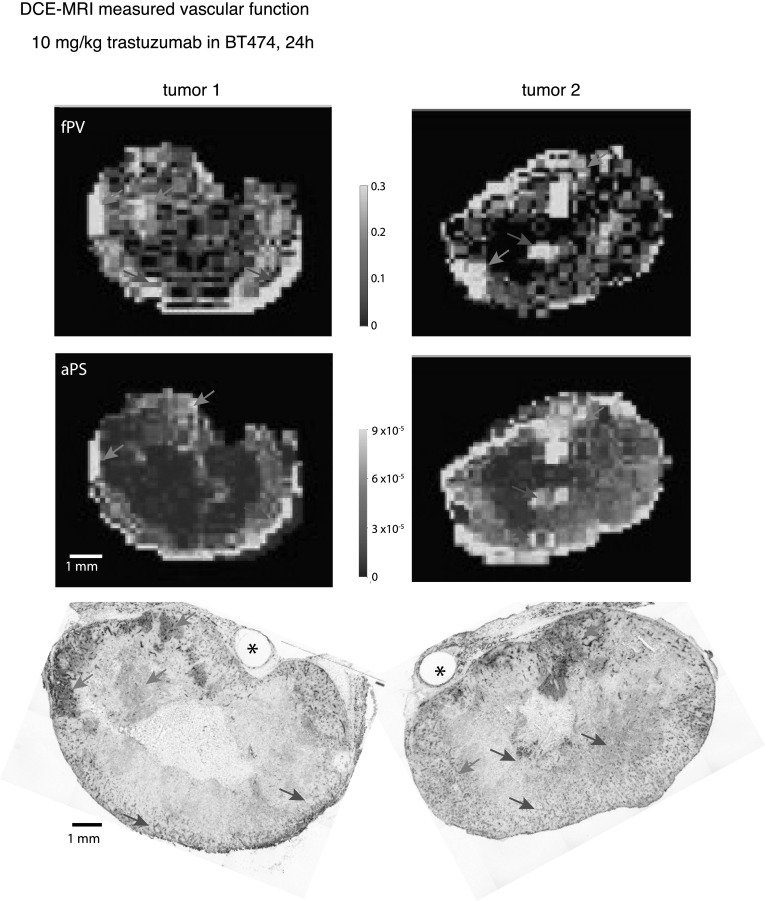
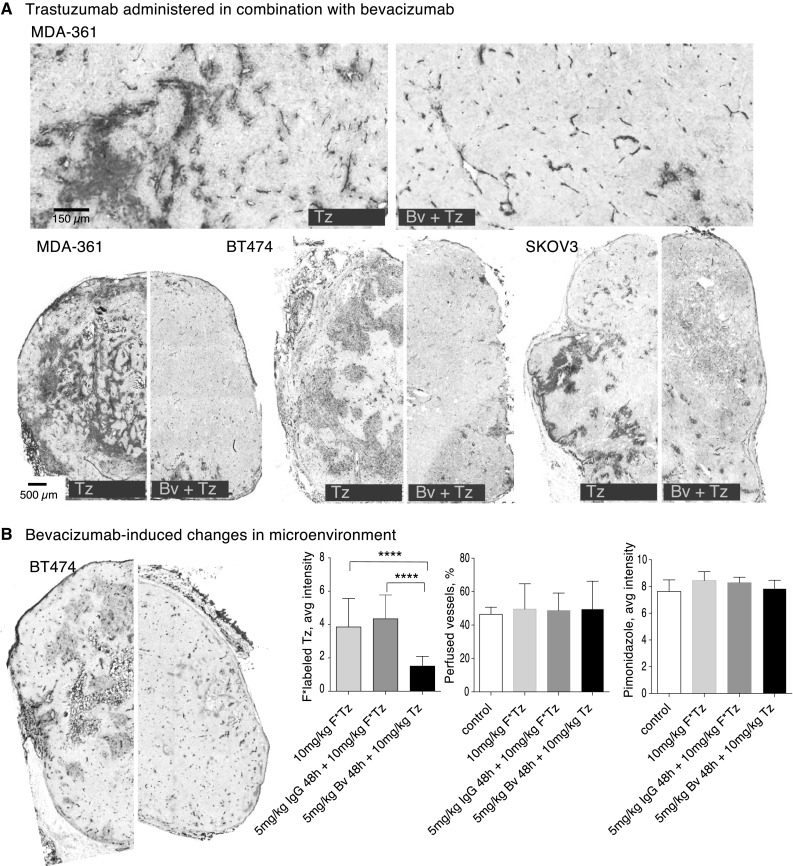
Most HER2-positive metastatic breast cancer patients continue to relapse. Incomplete access to all target HER2-positive cells in metastases and tumor tissues is a potential mechanism of resistance to trastuzumab. The location of locally bound trastuzumab was evaluated in HER2-positive tissues in vivo and as in vivo xenografts or metastases models in mice. Microenvironmental elements of tumors were related to bound trastuzumab using immunohistochemical staining and include tight junctions, vasculature, vascular maturity, vessel patency, hypoxia and HER2 to look for correlations. Trastuzumab was evaluated alone and in combination with bevacizumab. Dynamic contrast-enhanced magnetic resonance imaging parameters of overall vascular function, perfusion and apparent permeability were compared with matched histological images of trastuzumab distribution and vascular patency. Trastuzumab distribution is highly heterogeneous in all models examined, including avascular micrometastases of the brain and lung. Trastuzumab distributes well through the extravascular compartment even in conditions of high HER2 expression and poor convective flow in vivo. Microregional patterns of trastuzumab distribution in vivo do not consistently correlate with vascular density, patency, function or maturity; areas of poor trastuzumab access are not necessarily those with poor vascular supply. The number of vessels with perivascular trastuzumab increases with time and higher doses and dramatically decreases when pre-treated with bevacizumab. Areas of HER2-positive tissue without bound trastuzumab persist in all conditions. These data directly demonstrate tissue- and vessel-level barriers to trastuzumab distribution in vivo that can effectively limit access of the drug to target cells in brain metastases and elsewhere.
Keywords: Bevacizumab; Brain metastases; DCE-MRI; Drug distribution; HER2-positive metastases; HER2/neu; Herceptin; Monoclonal antibody therapeutic; Tumor microenvironment; Tumor vessel permeability.
Figures
Similar articles
-
Trastuzumab uptake and its relation to efficacy in an animal model of HER2-positive breast cancer brain metastasis.Breast Cancer Res Treat. 2017 Aug;164(3):581-591. doi: 10.1007/s10549-017-4279-4. Epub 2017 May 10. Breast Cancer Res Treat. 2017. PMID: 28493046 Free PMC article.
-
Positron-Emission Tomography of HER2-Positive Breast Cancer Xenografts in Mice with 89Zr-Labeled Trastuzumab-DM1: A Comparison with 89Zr-Labeled Trastuzumab.Mol Pharm. 2018 Aug 6;15(8):3383-3393. doi: 10.1021/acs.molpharmaceut.8b00392. Epub 2018 Jul 16. Mol Pharm. 2018. PMID: 29957952
-
Intrathecal Viral Vector Delivery of Trastuzumab Prevents or Inhibits Tumor Growth of Human HER2-Positive Xenografts in Mice.Cancer Res. 2018 Nov 1;78(21):6171-6182. doi: 10.1158/0008-5472.CAN-18-0363. Epub 2018 Aug 28. Cancer Res. 2018. PMID: 30154145
-
[Management of metastatic HER2-positive breast cancer: present and future].Bull Cancer. 2010 Mar;97(3):365-83. doi: 10.1684/bdc.2010.1040. Bull Cancer. 2010. PMID: 20176546 Review. French.
-
Pharmacokinetics of trastuzumab and its efficacy and safety in HER2-positive cancer patients.Cancer Chemother Pharmacol. 2024 Nov;94(5):721-732. doi: 10.1007/s00280-024-04707-y. Epub 2024 Aug 23. Cancer Chemother Pharmacol. 2024. PMID: 39177768 Review.
Cited by
-
Co-administered antibody improves penetration of antibody-dye conjugate into human cancers with implications for antibody-drug conjugates.Nat Commun. 2020 Nov 9;11(1):5667. doi: 10.1038/s41467-020-19498-y. Nat Commun. 2020. PMID: 33168818 Free PMC article. Clinical Trial.
-
A lactate-related LncRNA model for predicting prognosis, immune landscape and therapeutic response in breast cancer.Front Genet. 2022 Oct 5;13:956246. doi: 10.3389/fgene.2022.956246. eCollection 2022. Front Genet. 2022. PMID: 36276952 Free PMC article.
-
The root cause of drug resistance in HER2-positive breast cancer and the therapeutic approaches to overcoming the resistance.Pharmacol Ther. 2021 Feb;218:107677. doi: 10.1016/j.pharmthera.2020.107677. Epub 2020 Sep 6. Pharmacol Ther. 2021. PMID: 32898548 Free PMC article. Review.
-
Immune Cell Infiltration and Relevant Gene Signatures in the Tumor Microenvironment that Significantly Associates With the Prognosis of Patients With Breast Cancer.Front Mol Biosci. 2022 Feb 23;9:823911. doi: 10.3389/fmolb.2022.823911. eCollection 2022. Front Mol Biosci. 2022. PMID: 35281270 Free PMC article.
-
The Current Landscape of Antibody-based Therapies in Solid Malignancies.Theranostics. 2021 Jan 1;11(3):1493-1512. doi: 10.7150/thno.52614. eCollection 2021. Theranostics. 2021. PMID: 33391547 Free PMC article. Review.
References
-
- Bria E, Cuppone F, Fornier M, Nisticò C, Carlini P, Milella M, et al. Cardiotoxicity and incidence of brain metastases after adjuvant trastuzumab for early breast cancer: the dark side of the moon? A meta-analysis of the randomized trials. Breast Cancer Res Treat. 2008;109:231–239. doi: 10.1007/s10549-007-9663-z. - DOI - PubMed
-
- Murrell DH, Hamilton AM, Mallett CL, van Gorkum R, Chambers AF, Foster PJ. Understanding heterogeneity and permeability of brain metastases in murine models of HER2-positive breast cancer through magnetic resonance imaging: implications for detection and therapy. Transl Oncol. 2015;8:176–184. doi: 10.1016/j.tranon.2015.03.009. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
