

Multi-option therapy vs observation for small acoustic neuroma: hearing-focused management
- PMID: 30197430
- PMCID: PMC6146573
- DOI: 10.14639/0392-100X-1756
Multi-option therapy vs observation for small acoustic neuroma: hearing-focused management
Abstract
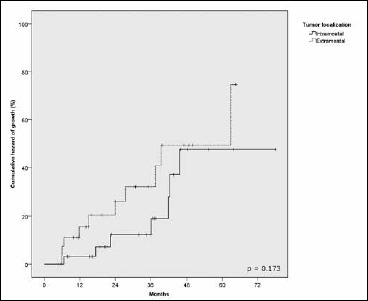
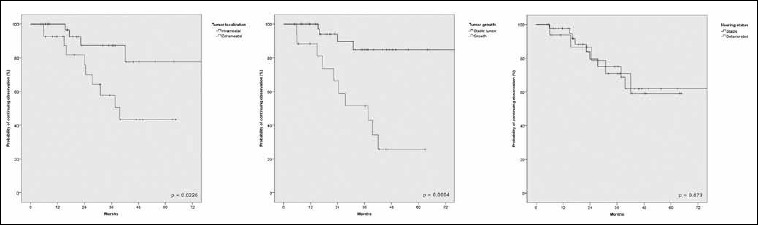
The current treatment options for acoustic neuromas (AN) - observation, microsurgery and radiotherapy - should assure no additional morbidity on cranial nerves VII and VIII. Outcomes in terms of disease control and facial function are similar, while the main difference lies in hearing. From 2012 to 2016, 91 of 169 patients (54%) met inclusion criteria for the present study, being diagnosed with unilateral, sporadic, intrameatal or extrameatal AN up to 1 cm in the cerebello-pontine angle; the remaining 78 patients (46%) had larger AN and were all addressed to surgery. The treatment protocol for small AN included observation, translabyrinthine surgery, hearing preservation surgery (HPS) and radiotherapy. Hearing function was assessed according to the Tokyo classification and the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS) classification. Sixty-one patients (71%) underwent observation, 19 (22%) HPS and 6 (7%) translabyrinthine surgery; 5 patients were lost to follow-up. Median follow-up was 25 months. In the observation group, 24.6% of patients abandoned the wait-and-see policy for an active treatment; the risk of switching from observation to active treatment was significant for tumour growth (p = 0.0035) at multivariate analysis. Hearing deteriorated in 28% of cases without correlation with tumour growth; the rate of hearing preservation for classes C-D was higher than for classes A-B (p = 0.032). Patients submitted to HPS maintained an overall preoperative hearing class of Tokyo and AAO-HNS in 63% and 68% of cases, respectively. Hearing preservation rate was significantly higher for patients presenting with preoperative favourable conditions (in-protocol) (p = 0.046). A multi-option management for small AN appeared to be an effective strategy in terms of hearing outcomes.
Opzioni di terapia vs osservazione per i piccoli neurinomi dell’acustico: una gestione orientata alla funzione uditiva.
Riassunto: Le opzioni di trattamento per il neurinoma del nervo acustico (AN), ovvero osservazione, microchirurgia e radioterapia non dovrebbero esporre a una morbidità addizionale i nervi cranici VII e VIII. Esse comportano risultati simili su controllo del tumore e conservazione del nervo facciale, ma differenti e discussi quanto a udito. Dal 2012 al 2016, 169 pazienti con diagnosi di AN sporadico, monolaterale sono stati valutati nel nostro centro. In totale, 91 pazienti hanno soddisfatto i criteri di inclusione, presentando un tumore intracanalare o extrameatale di dimensioni inferiori a 1 cm in angolo pontocerebellare. I restanti 78 pazienti con AN di dimensioni maggiori sono stati tutti trattati con opzione chirurgica primaria. La funzione uditiva è stata determinata sulla base delle classificazioni di Tokyo e dell’American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS). Il controllo post trattamento ha avuto una durata media di 25 mesi. Sessantuno pazienti (71%) sono andati incontro a trattamento conservativo di osservazione, 19 (22%) a chirurgia di preservazione dell’udito (HPS) e 6 (7%) a chirurgia per via translabirintica; 5 pazienti sono stati esclusi per incompletezza di dati. Il 24,6% dei pazienti in osservazione è uscito da tale protocollo durante il follow-up. Il rischio di cambiare da osservazione a trattamento attivo è risultato significativo all’analisi multivariata per i tumori in crescita (p = 0,0035). Nello stesso gruppo in osservazione, l’udito è andato incontro a un peggioramento nel 28% dei casi, indipendentemente da una correlazione con la crescita tumorale. La conservazione di un udito in classe A-B si è dimostrata significativamente inferiore rispetto a quella per un udito in classe C-D (p = 0,032) nel tempo di osservazione. I pazienti sottoposti a HPS hanno mantenuto la classe uditiva preoperatoria nel 63% e nel 68% dei casi, rispettivamente per le classificazioni di Tokyo e AAO-HNS. Il tasso di preservazione dell’udito inoltre, si è dimostrato significativamente maggiore per i pazienti che si presentavano con caratteristiche preoperatorie più favorevoli (in-protocol) (p = 0,046). Un protocollo di trattamento multi-opzionale per i piccoli AN rappresenta una strategia efficace per il risultato chirurgico a breve termine.
Keywords: Acoustic neuroma; Hearing preservation; Microsurgery; Vestibular schwannoma; Wait and see.
Copyright © 2018 Società Italiana di Otorinolaringologia e Chirurgia Cervico-Facciale, Rome, Italy.
Figures



References
-
- Stangerup SE, Caye-Thomasen P, Tos M, et al. The natural history of vestibular schwannoma. Otol Neurotol 2006;27:547-52. - PubMed
-
- Stangerup SE, Tos M, Thomsen J, et al. Hearing outcomes of vestibular schwannoma patients managed with ‘wait and scan’: predictive value of hearing level at diagnosis. J Laryngol Otol 2010;124:490-4. - PubMed
-
- Carlson ML, Link MJ, Wanna GB, et al. Management of sporadic vestibular schwannoma. Otolaryngol Clin North Am 2015;48:407-22. - PubMed
-
- Kirchmann M, Karnov K, Hansen S, et al. Ten-year follow-up on tumor growth and hearing in patients observed with an intracanalicular vestibular schwannoma. Neurosurgery 2017;80:49-56. - PubMed
-
- Golfinos JG, Hill TC, Rokosh R, et al. A matched cohort comparison of clinical outcomes following microsurgical resection or stereotactic radiosurgery for patients with small- and medium-sized vestibular schwannomas. J Neurosurg 2016;125:1472-82. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
