

Inequality in Care and Differences in Outcome Following Stroke in People With ESRD
- PMID: 30197973
- PMCID: PMC6127409
- DOI: 10.1016/j.ekir.2018.04.011
Inequality in Care and Differences in Outcome Following Stroke in People With ESRD
Abstract
Introduction: Stroke rate and mortality are greater in individuals with end-stage renal disease (ESRD) than in those without ESRD. We examined discrepancies in stroke care in ESRD patients and their influence on mortality.
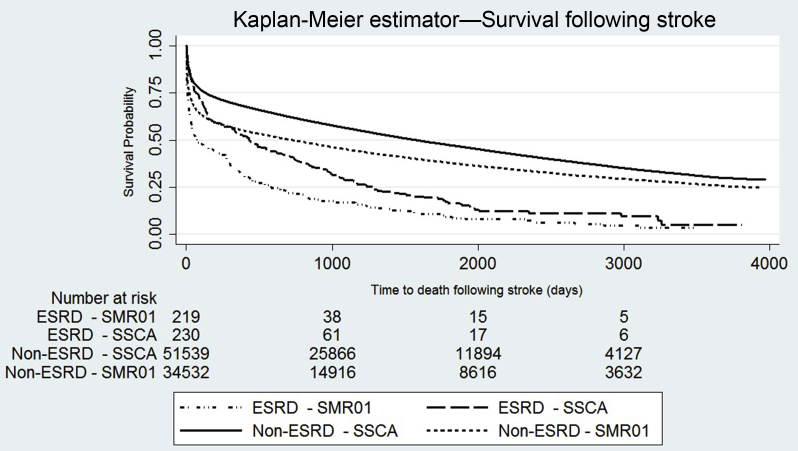
Methods: This is a national record linkage cohort study of hospitalized stroke individuals from 2005 to 2013. Presentation, measures of care quality (admission to stroke unit, swallow assessment, antithrombotics, or thrombolysis use), and outcomes were compared in those with and without ESRD after propensity score matching (PSM). We examined the effect of being admitted to a stroke unit on survival using Kaplan-Meier and Cox survival analyses.
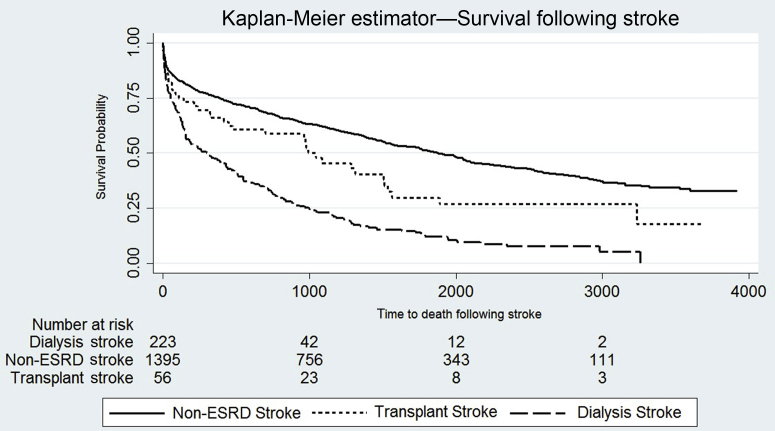
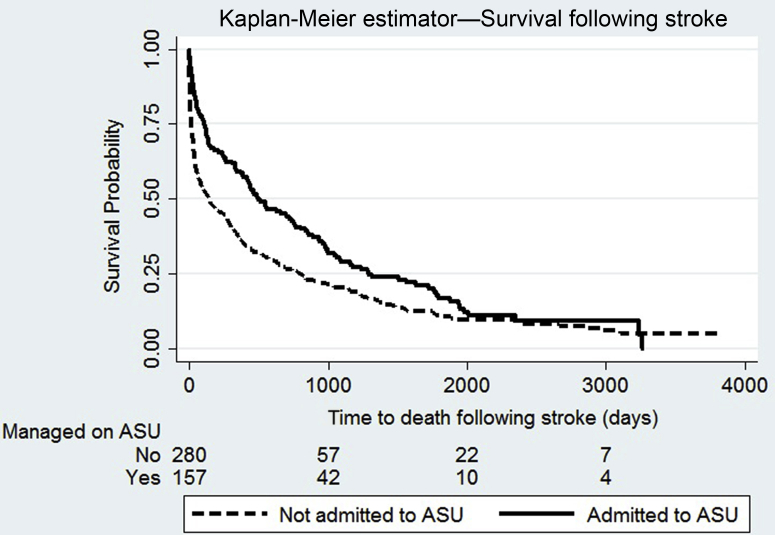
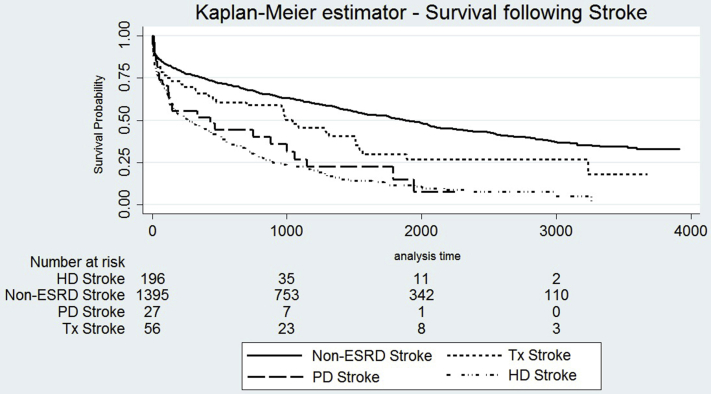
Results: A total of 8757 individuals with ESRD and 61,367 individuals with stroke were identified. ESRD patients (n =486) experienced stroke over 34,551.9 patient-years of follow-up; incidence rates were 25.3 (dialysis) and 4.5 (kidney transplant)/1000 patient-years. After PSM, dialysis patients were less likely to be functionally independent (61.4% vs. 77.7%; P < 0.0001) before stroke, less frequently admitted to stroke units (64.6% vs. 79.6%; P < 0.001), or to receive aspirin (75.3% vs. 83.2%; P = 0.01) than non-ESRD stroke patients. There were no significant differences in management of kidney transplantation patients. Stroke with ESRD was associated with a higher death rate during admission (dialysis 22.9% vs.14.4%, P = 0.002; transplantation: 19.6% vs. 9.3%; P = 0.034). Managing ESRD patients in a stroke unit was associated with a lower risk of death at follow-up (hazard ratio: 0.68; 95% confidence interval: 0.55-0.84).
Conclusion: Stroke incidence is high in ESRD. Individuals on dialysis are functionally more dependent before stroke and less frequently receive optimal stroke care. After a stroke, death is more likely in ESRD patients. Acute stroke unit care may be associated with lower mortality.
Keywords: ESRD; dialysis; stroke; transplantation outcomes.
Figures
References
-
- Gansevoort R.T., Correa-Rotter R., Hemmelgarn B.R. Chronic kidney disease and cardiovascular risk: epidemiology, mechanisms, and prevention. Lancet. 2013;382:339–352. - PubMed
-
- JBS3 Board Joint British Societies’ consensus recommendations for the prevention of cardiovascular disease (JBS3) Heart. 2014;100:ii1–ii67. - PubMed
-
- Foley R.N., Parfrey P.S., Sarnak M.J. Epidemiology of cardiovascular disease in chronic renal disease. J Am Soc Nephrol. 1998;9:S16–S23. - PubMed
-
- de Jager D.J., Grootendorst D.C., Jager K.J. Cardiovascular and noncardiovascular mortality among patients starting dialysis. JAMA. 2009;302:1782–1789. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
