

Soluble Urokinase Plasminogen Activator Receptor (suPAR) and All-Cause and Cardiovascular Mortality in Diverse Hemodialysis Patients
- PMID: 30197976
- PMCID: PMC6127402
- DOI: 10.1016/j.ekir.2018.05.004
Soluble Urokinase Plasminogen Activator Receptor (suPAR) and All-Cause and Cardiovascular Mortality in Diverse Hemodialysis Patients
Abstract
Introduction: The soluble receptor of urokinase plasminogen activator (suPAR) is an innate immunity/inflammation biomarker predicting cardiovascular (CV) and non-CV events in various conditions, including type 2 diabetic patients on dialysis. However, the relationship between suPAR and clinical outcomes in the hemodialysis population at large has not been tested.
Methods: We measured plasma suPAR levels (R&D enzyme-linked immunosorbent assay [ELISA]) in 1038 hemodialysis patients with a follow-up of 2.9 years (interquartile range = 1.7-4.2) who were enrolled in the PROGREDIRE study, a cohort study involving 35 dialysis units in 2 regions in Southern Italy.
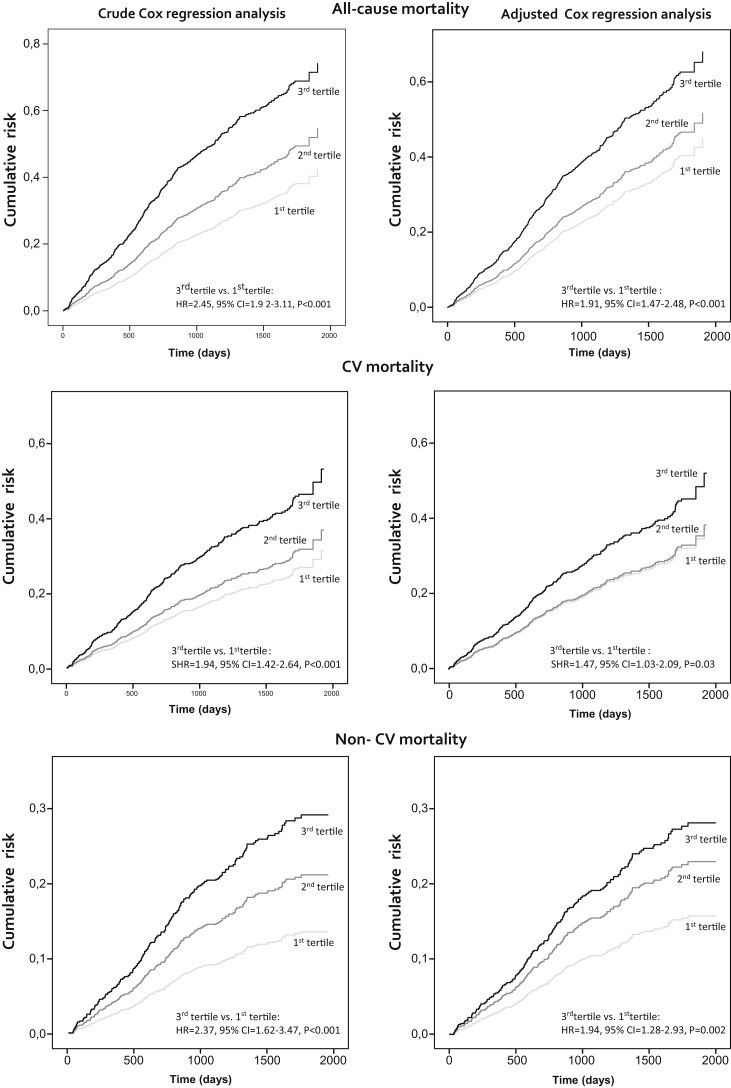
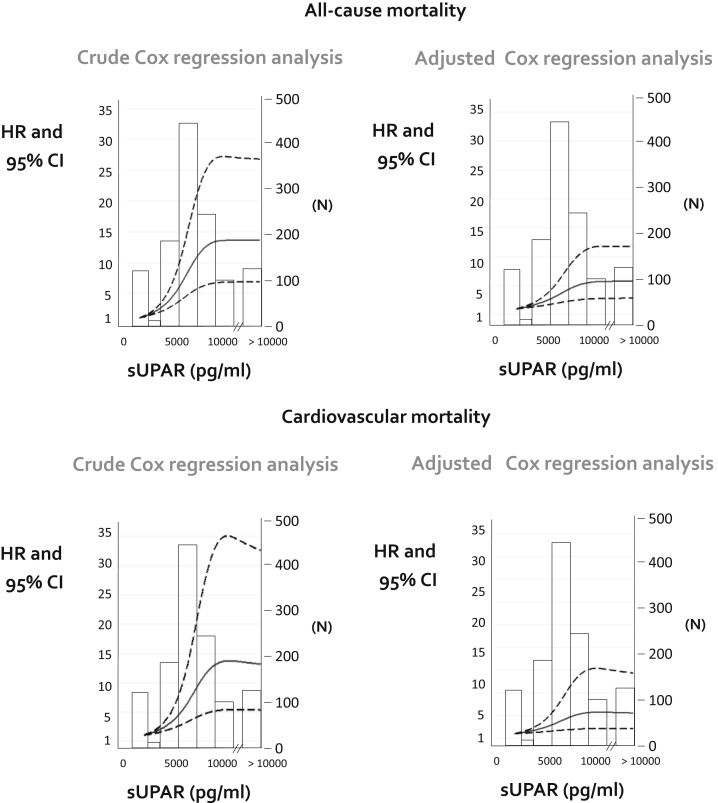
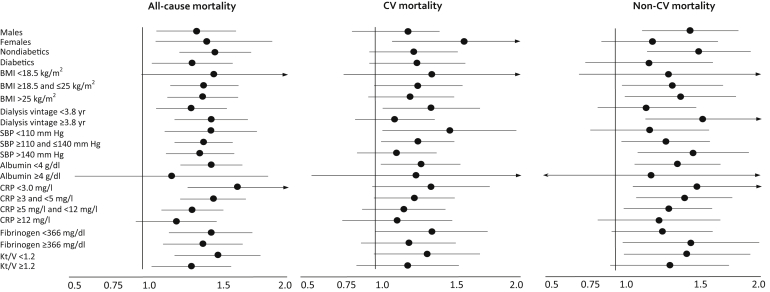
Results: suPAR was strongly (P < 0.001) and independently related to female gender (β = -0.160), age (β = 0.216), dialysis vintage (β = 0.264), CV comorbidities (β = 0.105), alkaline phosphatase (β = 0.136), albumin (β = -0.147), and body mass index (BMI; β = 0.174) (all P < 0.006). In fully adjusted analyses, suPAR tertiles predicted the risk of all-cause mortality (third tertile vs. first tertile hazard ratio (HR) = 1.91, 95% confidence interval (CI) = 1.47 - 2.48, P < 0.001), CV mortality (HR = 1.47, 95% CI = 1.03-2.09, P = 0.03), and non-CV mortality (HR = 1.94, 95% CI = 1.28-2.93, P = 0.002); these relationships were not modified by diabetes or other risk factors. suPAR added only modest prognostic risk discrimination and reclassification power for these outcomes to parsimonious models based on simple clinical variables.
Conclusion: In conclusion, suPAR robustly predicted all-cause and both CV and non-CV mortality in a large unselected hemodialysis population. Intervention studies are needed to definitively test the hypothesis that suPAR is causally implicated in clinical outcomes in this population.
Keywords: cardiovascular mortality; hemodialysis; mortality; noncardiovascular mortality; soluble urokinase plasminogen activator receptor (suPAR).
Figures
References
-
- Liyanage T., Ninomiya T., Jha V. Worldwide access to treatment for end-stage kidney disease: a systematic review. Lancet. 2015;385:1975–1982. - PubMed
-
- USRDS. 2015 USRDS annual data report volume 2: ESRD in the United States. 2016;2:1–274.
-
- Kramann R., Floege J., Ketteler M. Medical options to fight mortality in end-stage renal disease: a review of the literature. Nephrol Dial Transplant. 2012;27:4298–4307. - PubMed
-
- Ortiz A., Covic A., Fliser D. Epidemiology, contributors to, and clinical trials of mortality risk in chronic kidney failure. Lancet. 2014;383:1831–1843. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
