

Impact of pregnancy on inborn errors of metabolism
- PMID: 30198059
- PMCID: PMC6208575
- DOI: 10.1007/s11154-018-9455-2
Impact of pregnancy on inborn errors of metabolism
Abstract
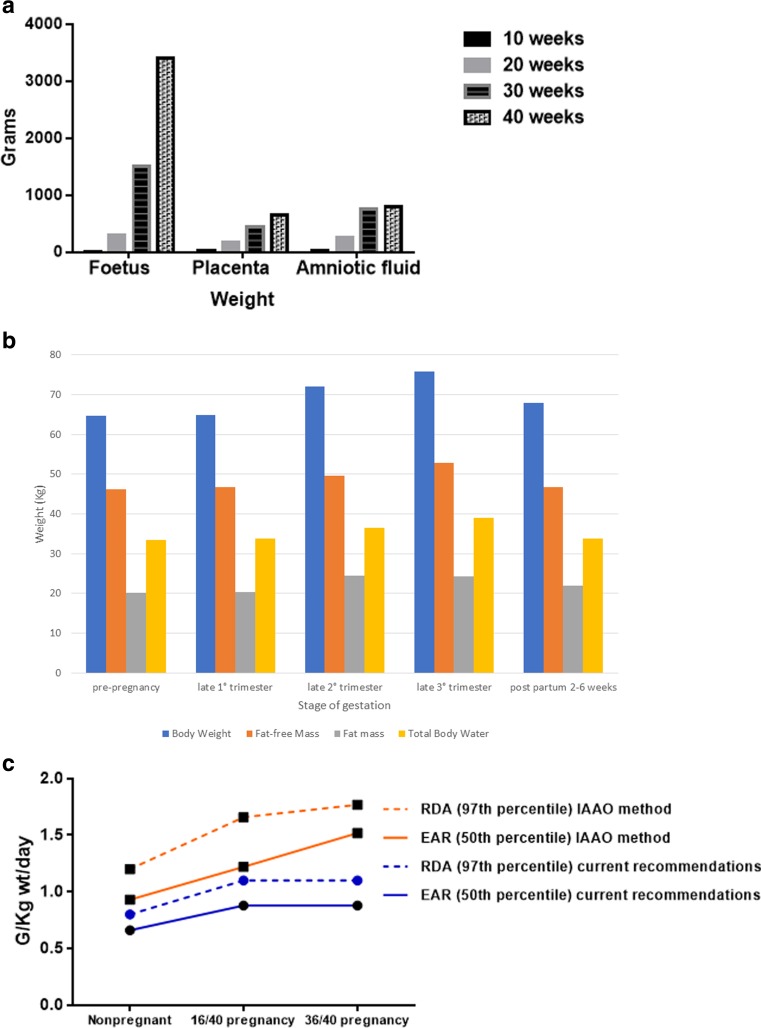
Once based mainly in paediatrics, inborn errors of metabolism (IEM), or inherited metabolic disorders (IMD) represent a growing adult medicine specialty. Individually rare these conditions have currently, a collective estimated prevalence of >1:800. Diagnosis has improved through expanded newborn screening programs, identification of potentially affected family members and greater awareness of symptomatic presentations in adolescence and in adulthood. Better survival and reduced mortality from previously lethal and debilitating conditions means greater numbers transition to adulthood. Pregnancy, once contraindicated for many, may represent a challenging but successful outcome. Successful pregnancies are now reported in a wide range of IEM. Significant challenges remain, given the biological stresses of pregnancy, parturition and the puerperium. Known diagnoses allow preventive and pre-emptive management. Unrecognized metabolic disorders especially, remain a preventable cause of maternal and neonatal mortality and morbidity. Increased awareness of these conditions amongst all clinicians is essential to expedite diagnosis and manage appropriately. This review aims to describe normal adaptations to pregnancy and discuss how various types of IEM may be affected. Relevant translational research and clinical experience will be reviewed with practical management aspects cited. Based on current literature, the impact of maternal IEM on mother and/or foetus, as well as how foetal IEM may affect the mother, will be considered. Insights gained from these rare disorders to more common conditions will be explored. Gaps in the literature, unanswered questions and steps to enhance further knowledge and systematically capture experience, such as establishment of an IEM-pregnancy registry, will be summarized.
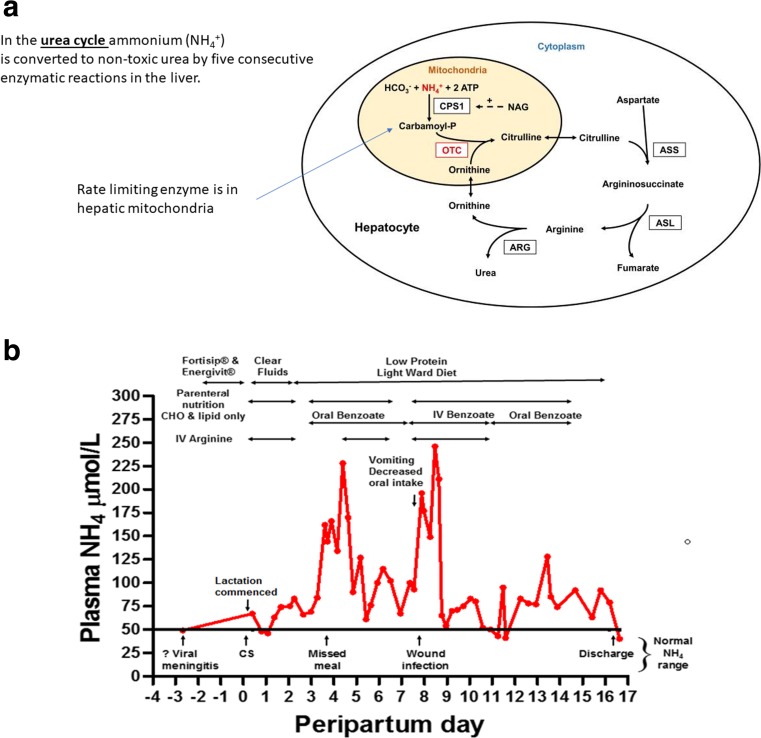
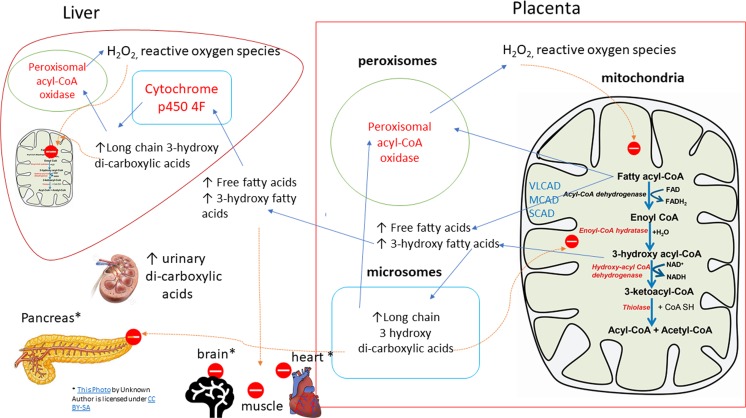
Keywords: Fatty acid oxidation; Inborn errors of metabolism; Metabolic disorders; Mitochondrial; Pregnancy; Urea cycle.
Conflict of interest statement
Conflict of interest
The author has received travel grants from Genzyme, Biomarin, Alexion and Shire, speaker honoraria from Vitaflo, Biomarin, Shire and Nutricia, research grants from the MPS society (UK), and advisory board membership with Biomarin, Medical Advisory Panel membership for the National Society for PKU (NSPKU) and consultancies for Dimension Therapeutics.
Informed consent
Informed consent was obtained from those individuals presented in case reports cited and authored by the author. Identifiable individual data has been removed from unpublished data presented.
Figures
References
-
- Hollak C, Lachmann R. In: Hollak C, Lachmann R, editors. Inherited metabolic disease in adults: a clinical guide (Oxford monographs on medical genetics). Oxford: Oxford University Press; 2016. p. xiii–ix.
-
- Erikson EH, editor. Youth: change and challenge. New York: Basic Books; 1963.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
