

Maintenance of low disease activity and remission with etanercept-disease-modifying antirheumatic drug (DMARD) combination therapy compared with treatment with DMARDs alone in Latin American patients with active rheumatoid arthritis: Subset analysis of a randomized trial
- PMID: 30200078
- PMCID: PMC6133462
- DOI: 10.1097/MD.0000000000011989
Maintenance of low disease activity and remission with etanercept-disease-modifying antirheumatic drug (DMARD) combination therapy compared with treatment with DMARDs alone in Latin American patients with active rheumatoid arthritis: Subset analysis of a randomized trial
Abstract
Background: Current guidelines on the treatment of rheumatoid arthritis (RA) recommend early therapy targeting the achievement of low disease activity (LDA) or clinical remission. Little published information is available on the success of this treatment strategy in Latin America. In a subset analysis of patients from Latin America, we compared efficacy maintenance with etanercept 50 mg once weekly (ETN50) versus placebo (PBO), on a background of methotrexate (MTX) ± other non-biologic, disease-modifying antirheumatic drugs, in patients with moderate-to-severe RA who had achieved LDA with ETN50.
Methods: In the Treat-to-Target trial, adult patients with active RA nonresponsive to MTX were treated with ETN50 for 24 weeks (Period 1). Patients achieving LDA were randomized to receive ETN50 or PBO for 28 additional weeks (Period 2). The proportion of patients maintaining LDA at week 52 and other efficacy and quality-of-life measures were assessed. Descriptive statistics are presented using last observation carried forward imputation of data.
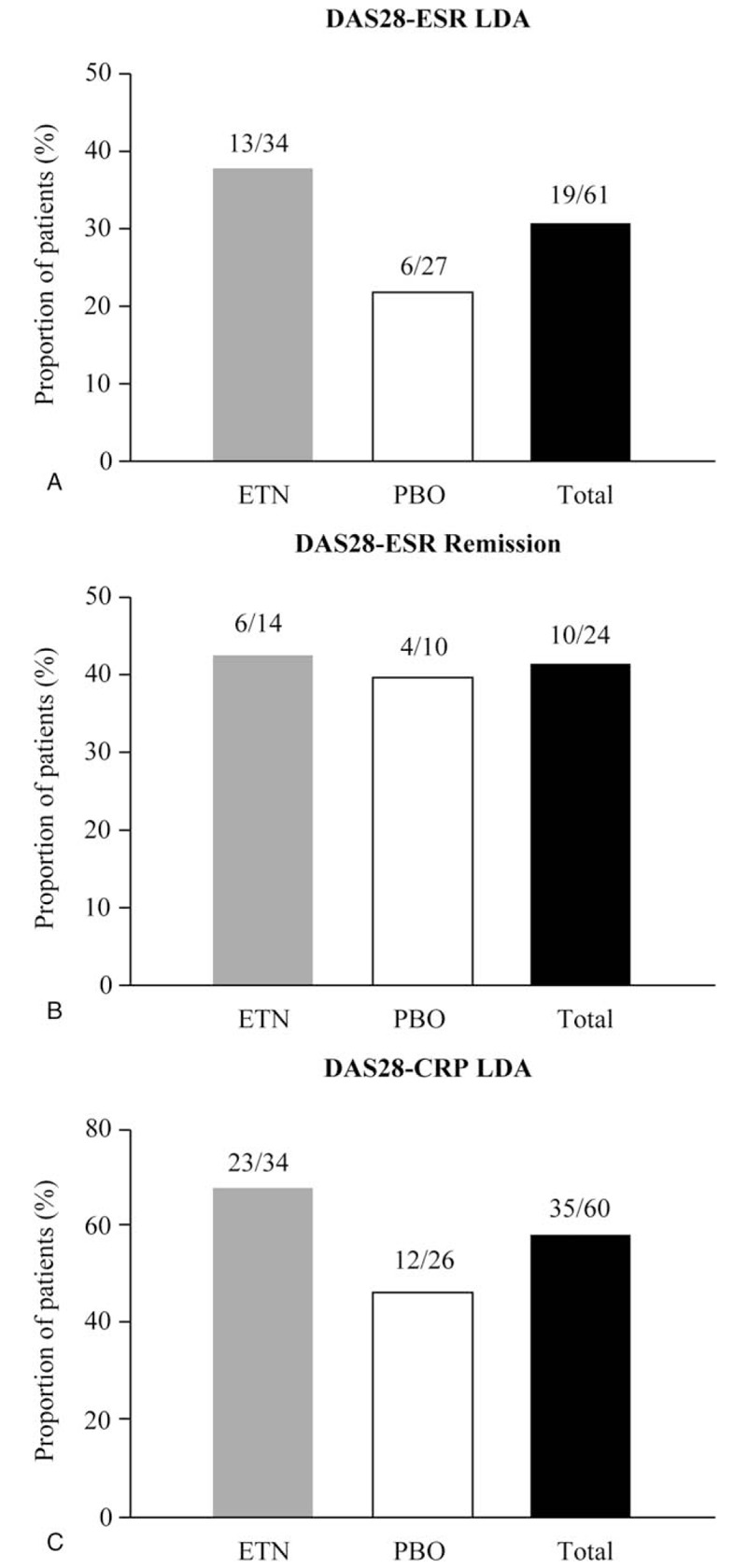
Results: Of the 64 patients from Latin America treated in Period 1, 61 (95.3%) achieved LDA. Among patients receiving ETN50, 13/34 remained in LDA and 6/14 maintained remission at week 52 versus 6/27 and 4/10 patients receiving PBO. The median time to flare was 113 days and 33 days for the ETN50 and PBO groups, respectively. In the overall population, adverse events were reported in 37% and 43%, serious adverse events in 1% and 4%, and serious infections in 0% and 2% of patients in the ETN50 and PBO groups, respectively.
Conclusions: In patients with RA from Latin America, continuing treatment with ETN50 after achieving LDA appears to result in a higher proportion of patients maintaining LDA and remission compared with switching to PBO. CLINICALTRIALS.
Gov registration: NCT01578850.
Figures

References
-
- Halabi H, Alarfaj A, Alawneh K, et al. Challenges and opportunities in the early diagnosis and optimal management of rheumatoid arthritis in Africa and the Middle East. Int J Rheum Dis 2015;18:268–75. - PubMed
-
- Kourilovitch M, Galarza-Maldonado C, Ortiz-Prado E. Diagnosis and classification of rheumatoid arthritis. J Autoimmun 2014;48–49:26–30. - PubMed
-
- Mody GM, Cardiel MH. Challenges in the management of rheumatoid arthritis in developing countries. Best Pract Res Clin Rheumatol 2008;22:621–41. - PubMed
-
- Conti F, Ceccarelli F, Massaro L, et al. Biological therapies in rheumatic diseases. Clin Ter 2013;164:e413–28. - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
