

Paraneoplastic immunoglobulin A nephropathy and associated focal segmental glomerulosclerosis in asymptomatic low volume B-cell lymphoma - a case report
- PMID: 30200898
- PMCID: PMC6131739
- DOI: 10.1186/s12882-018-1034-y
Paraneoplastic immunoglobulin A nephropathy and associated focal segmental glomerulosclerosis in asymptomatic low volume B-cell lymphoma - a case report
Abstract
Background: Paraneoplastic glomerulonephritis is rare in haematological malignancies and tends to manifest as minimal change disease, membranous glomerulonephritis or membranoproliferative glomerulonephritis. We present the first report of immunoglobulin A nephropathy and associated focal segmental glomerulosclerosis in a patient with asymptomatic low grade B-cell lymphoma.
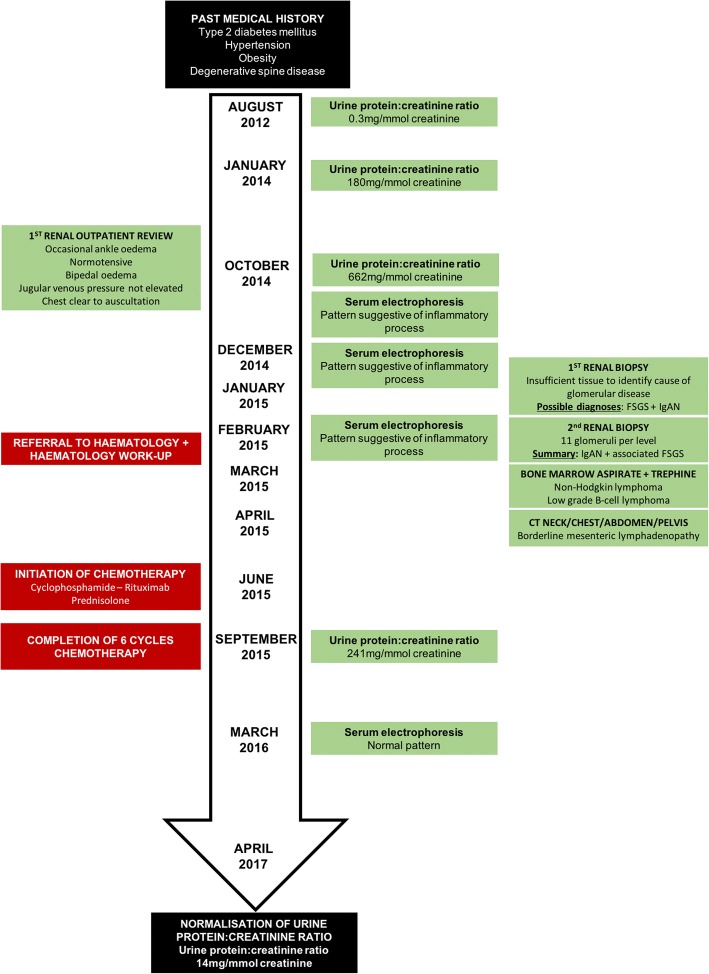
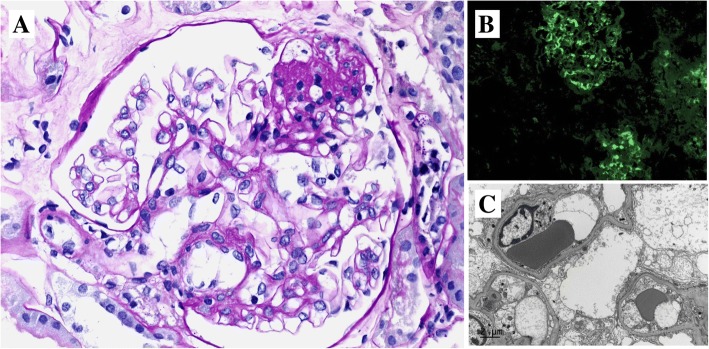
Case presentation: A 53 year old gentleman presented with nephrotic range proteinuria (urine protein creatinine ratio of 662 mg/mmol) on a background of type 2 diabetes mellitus (glycosylated haemoglobin: < 6%), hypertension, obesity (body mass index: 47.6 kg/m2) and degenerative spine disease. Bone marrow biopsy diagnosed a low grade B-cell lymphoma and renal biopsy was consistent with immunoglobulin A nephropathy. Lymphoma treatment with six cycles of cyclophosphamide/ rituximab/ prednisolone led to normalisation of urinary protein excretion (urine protein creatinine ratio: 14 mg/mmol at 26 months post-chemotherapy).
Conclusion: Paraneoplastic immunoglobulin A nephropathy can occur with a broad range of haematological malignancies regardless of stage. This case illustrates the importance of meticulous haematological system work-up for patients presenting with immunoglobulin A nephropathy. Recognition of paraneoplastic immunoglobulin A nephropathy and early diagnosis of associated malignancy can be life-saving.
Keywords: Glomerulonephritis; Immunoglobulin A nephropathy; Lymphoma; Non-Hodgkin; Paraneoplastic; Proteinuric.
Conflict of interest statement
Ethical approval and consent to participate
Not applicable.
Consent for publication
Written consent was obtained from the patient for publication of case report and any accompanying images.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
