

Evaluation of neonatal and maternal morbidity in mothers with gestational diabetes: a population-based study
- PMID: 30200916
- PMCID: PMC6131836
- DOI: 10.1186/s12884-018-2005-9
Evaluation of neonatal and maternal morbidity in mothers with gestational diabetes: a population-based study
Abstract
Background: Gestational diabetes mellitus (GDM) is the most frequent complication during pregnancy. Untreated GDM is a severe threat to maternal and neonatal health. Based on recent evidence, up to 15% of all pregnancies may be affected by GDM. We hypothesized that in a rural birth cohort, higher maternal BMI and adverse socioeconomic conditions would promote GDM, which in turn would lead to adverse effects on pregnancy outcomes.
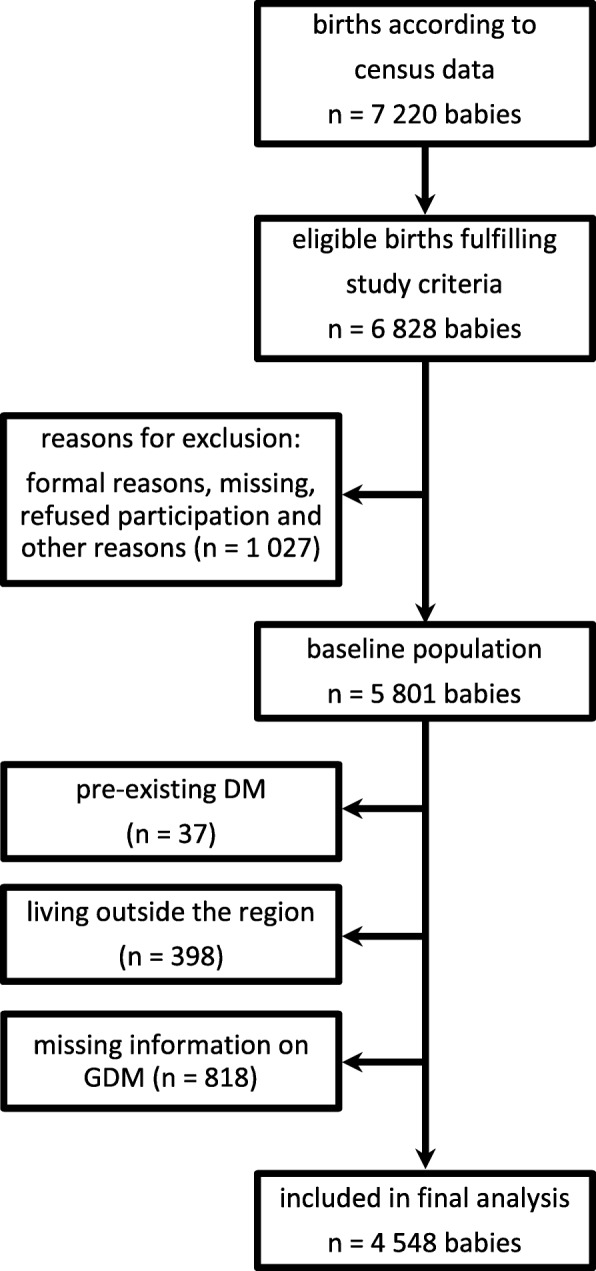
Methods: The current study is a part of a population-based cohort study examining the health and socioeconomic information from 5801 mothers and their children. The study, titled the Survey of Neonates in Pomerania (SNiP), was based in northeastern Pomerania, Germany (2002-2008).
Results: The cumulative incidence of GDM was 5.1%. Multiple logistic regression revealed prepregnancy overweight (OR 1.84 (95% CI 1.27-2.68)), prepregnancy obesity (OR 3.67 (2.48-5.44)) and maternal age (OR 1.06 (1.03-1.08)) as risk factors for GDM (p = 0.001). Alcohol use during pregnancy (OR 0.61 (0.41-0.90), a higher monthly income (OR 0.62 (0.46-0.83)), and the highest level of education (OR 0.44 (0.46-0.83)) decreased the risk of GDM. Newborns of GDM mothers had an increased risk of hypoglycaemia (OR 11.71 (7.49-18.30)) or macrosomia (OR 2.43 (1.41-4.18)) and were more often delivered by primary (OR 1.76 (1.21-2.60)) or secondary C-section (OR 2.00 (1.35-2.97)). Moreover, they were born 0.78 weeks (95% CI -1.09 - -0.48 weeks) earlier than infants of mothers without diabetes, resulting in higher percentage of late preterm infants with a gestational age of 32-36 weeks (11.1% vs. 6.96%).
Conclusions: Age and BMI before pregnancy were the predominant mediators of the increased risk of GDM, whereas a higher income and educational level were protective. GDM affected relevant perinatal and neonatal outcomes based on its association with an increased risk of delivery by C-section, preterm birth, macrosomia at birth and neonatal hypoglycaemia.
Keywords: Gestational diabetes mellitus; Pregnancy; Risk factors; SNiP; Survey of neonates in Pomerania.
Conflict of interest statement
Ethics approval and consent to participate
Research based on patient-related data and human DNA is strictly regulated by German law. The collection of detailed personal data, combined with the sampling of biomaterials, demands strict confidentiality. Our study complies with international guidelines of ethical research based on the Declaration of Helsinki. The study design was reviewed and approved by the Ethics Committee of the Board of Physicians Mecklenburg-Western Pomerania at the University of Greifswald (Reg.-Nr. III UV 20/00). Eligible women were asked for written informed consent; in cases of legally minor mothers, i.e., aged < 18 years, the additional signatures of the newborn’s and legally minor mother’s legal caregivers were required. The enrolment procedure was described in details by Ebner and colleagues [23]. The written informed consent form included data assessment in face-to-face interviews, self-administered questionnaires and patient records. It also covered biosamples of blood. Furthermore, informed consent covered the storage of pseudonymized data as well as their analyses and publication.
The current study is a part of a population-based birth cohort `Survey of Neonates in Pomerania´ (SNiP) examining the health and socioeconomic information from 5801 mothers and their children. SNiP was designed as a multi-purpose birth cohort to serve as a platform for studies of pregnancy complications, maternal and child health from pregnancy through to adulthood after completion of follow up. Therefore, all analyses from this database have to be regarded as secondary analyses.
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Kleinwechter H, Schäfer-Graf U, Bührer C, Hoesli I, Kainer F, Kautzky-Willer A, et al. Gestationsdiabetes mellitus (GDM): Evidenzbasierte Leitlinie zu Diagnostik, Therapie u. Nachsorge der Deutschen Diabetes-Gesellschaft (DDG) und der Deutschen Gesellschaft für Gynäkologie und Geburtshilfe (DGGG); 2011.
-
- AQUA – Institut für angewandte Qualitätsförderung und Forschung im Gesundheitswesen GmbH. Bundesauswertung zum Verfahrensjahr 2010 16/1 – Geburtshilfe Qualitätsindikatoren.: Erstellt am: 15.06.2011–21/201120003; 2011.
-
- International Diabetes Federation . IDF diabetes atlas. Brussels: International Diabetes Federation; 2015.
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
