

The Terry Fox Research Institute Canadian Prostate Cancer Biomarker Network: an analysis of a pan-Canadian multi-center cohort for biomarker validation
- PMID: 30200929
- PMCID: PMC6131811
- DOI: 10.1186/s12894-018-0392-x
The Terry Fox Research Institute Canadian Prostate Cancer Biomarker Network: an analysis of a pan-Canadian multi-center cohort for biomarker validation
Abstract
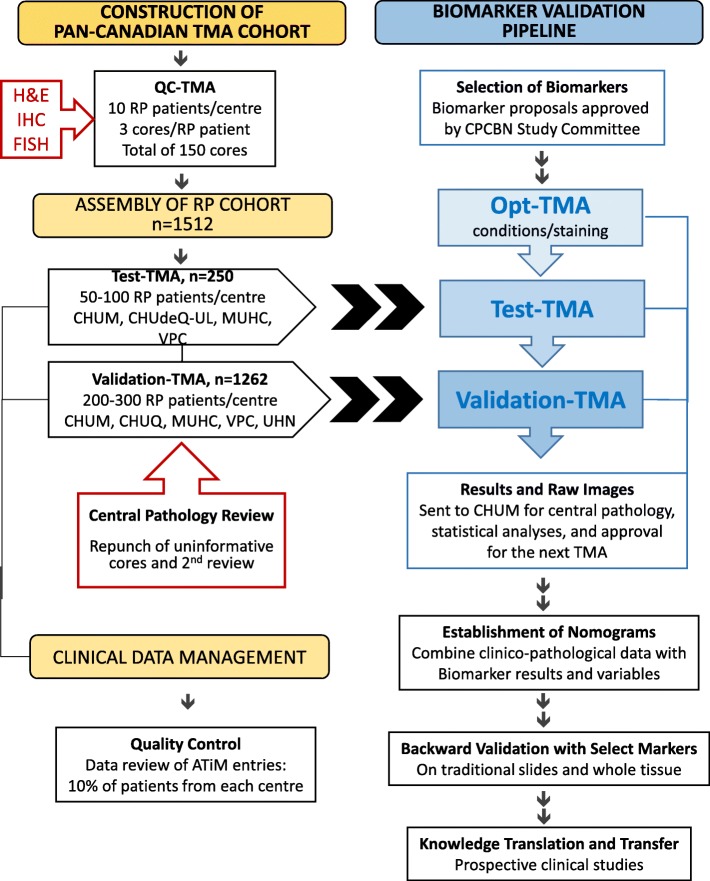
Background: Refinement of parameters defining prostate cancer (PC) prognosis are urgently needed to identify patients with indolent versus aggressive disease. The Canadian Prostate Cancer Biomaker Network (CPCBN) consists of researchers from four Canadian provinces to create a validation cohort to address issues dealing with PC diagnosis and management.
Methods: A total of 1512 radical prostatectomy (RP) specimens from five different biorepositories affiliated with teaching hospitals were selected to constitute the cohort. Tumoral and adjacent benign tissues were arrayed on tissue microarrays (TMAs). A patient clinical database was developed and includes data on diagnosis, treatment and clinical outcome.
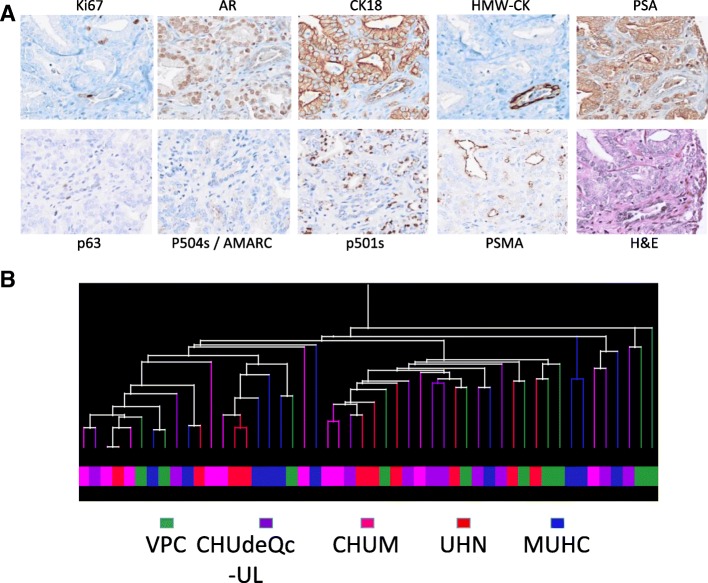
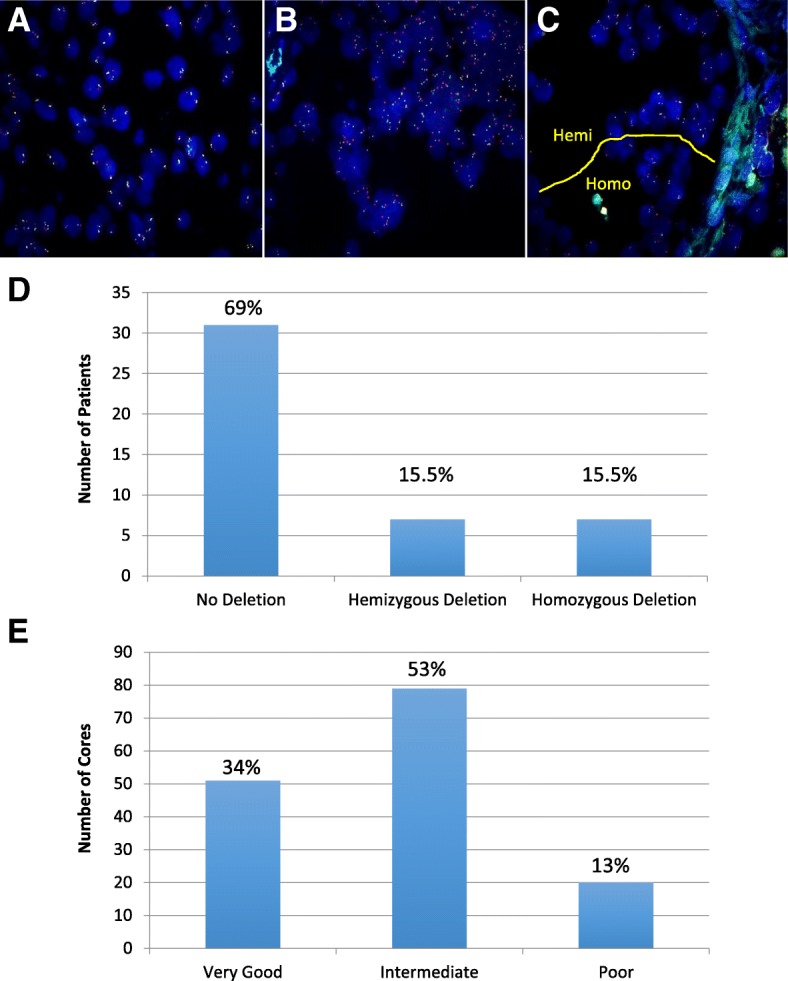
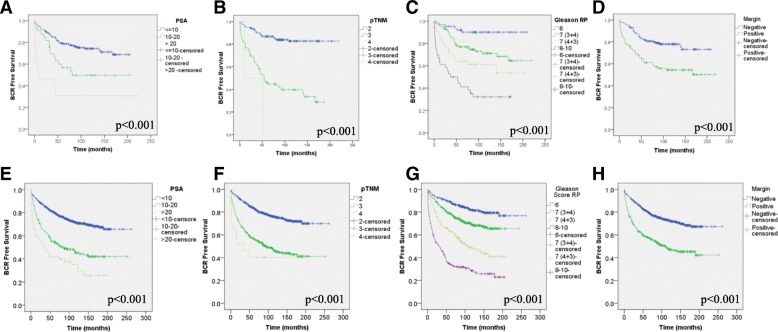
Results: Mean age at diagnosis of patients in the cohort was 61 years. Of these patients, 31% had a low grade (≤6) Gleason score (GS), 55% had GS 7 (40% of 3 + 4 and 15% of 4 + 3) and 14% had high GS (≥8) PC. The median follow-up of the cohort was 113 months. A total of 34% had a biochemical relapse, 4% developed bone metastasis and 3% of patients died from PC while 9% died of other causes. Pathological review of the TMAs confirmed the presence of tumor and benign tissue cores for > 94% of patients. Immunohistochemistry and FISH analyses, performed on a small set of specimens, showed high quality results and no biorepository-specific bias.
Conclusions: The CPCBN RP cohort is representative of real world PC disease observed in the Canadian population. The frequency of biochemical relapse and bone metastasis as events allows for a precise assessment of the prognostic value of biomarkers. This resource is available, in a step-wise manner, for researchers who intend to validate prognostic biomarkers in PC. Combining multiple biomarkers with clinical and pathologic parameters that are predictive of outcome will aid in clinical decision-making for patients treated for PC.
Keywords: Biomarker validation; Immunohistochemistry; Patient prognosis; Prostate cancer; Tissue microarray.
Conflict of interest statement
Ethics approval and consent to participate
Research ethics approval was obtained from each of the participating sites: the Centre de recherche du Centre hospitalier de l’Université de Montréal (CRCHUM), CHU de Québec-Université Laval (CHUdeQ-UL), McGill University Health Centre (MUHC), Vancouver Prostate Centre (VPC), and University Health Network (UHN). All patients signed an informed consent to participate within one of the biobanks and agreed to the use of their specimens and data for research purposes.
Consent for publication
Not applicable
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
Similar articles
-
Validation of the prognostic value of NF-κB p65 in prostate cancer: A retrospective study using a large multi-institutional cohort of the Canadian Prostate Cancer Biomarker Network.PLoS Med. 2019 Jul 2;16(7):e1002847. doi: 10.1371/journal.pmed.1002847. eCollection 2019 Jul. PLoS Med. 2019. PMID: 31265453 Free PMC article.
-
New Prostate Cancer Grading System Predicts Long-term Survival Following Surgery for Gleason Score 8-10 Prostate Cancer.Eur Urol. 2017 Jun;71(6):907-912. doi: 10.1016/j.eururo.2016.11.006. Epub 2016 Nov 19. Eur Urol. 2017. PMID: 27876305
-
Validation of lymphovascular invasion is an independent prognostic factor for biochemical recurrence after radical prostatectomy.Urol Oncol. 2016 May;34(5):233.e1-6. doi: 10.1016/j.urolonc.2015.10.013. Epub 2016 Mar 10. Urol Oncol. 2016. PMID: 26973136
-
A model for the design and construction of a resource for the validation of prognostic prostate cancer biomarkers: the Canary Prostate Cancer Tissue Microarray.Adv Anat Pathol. 2013 Jan;20(1):39-44. doi: 10.1097/PAP.0b013e31827b665b. Adv Anat Pathol. 2013. PMID: 23232570 Free PMC article. Review.
-
Prognostic histopathological and molecular markers on prostate cancer needle-biopsies: a review.Biomed Res Int. 2014;2014:341324. doi: 10.1155/2014/341324. Epub 2014 Aug 27. Biomed Res Int. 2014. PMID: 25243131 Free PMC article. Review.
Cited by
-
Optimization of tissue microarray technique for breast cancer patients: a short communication.Ann Med Surg (Lond). 2023 Sep 1;85(10):5299-5303. doi: 10.1097/MS9.0000000000001230. eCollection 2023 Oct. Ann Med Surg (Lond). 2023. PMID: 37811076 Free PMC article.
-
Optimization of Tissue Microarrays from Banked Human Formalin-Fixed Paraffin Embedded Tissues in the Cancer Research Setting.Biopreserv Biobank. 2019 Oct;17(5):452-457. doi: 10.1089/bio.2019.0011. Epub 2019 Jun 13. Biopreserv Biobank. 2019. PMID: 31194582 Free PMC article.
-
2018 CUA Abstracts.Can Urol Assoc J. 2018 Jun;12(6Suppl2):S51-S136. Can Urol Assoc J. 2018. PMID: 29877793 Free PMC article. No abstract available.
-
Building a Canadian Translational Bladder Cancer Research Network.Can Urol Assoc J. 2020 Oct;14(10):E475-E481. doi: 10.5489/cuaj.6887. Can Urol Assoc J. 2020. PMID: 33275556 Free PMC article. No abstract available.
-
A Novel Six-Gene Signature for Prognosis Prediction in Ovarian Cancer.Front Genet. 2020 Oct 15;11:1006. doi: 10.3389/fgene.2020.01006. eCollection 2020. Front Genet. 2020. PMID: 33193589 Free PMC article.
References
-
- Huber F, Montani M, Sulser T, Jaggi R, Wild P, Moch H, et al. Comprehensive validation of published immunohistochemical prognostic biomarkers of prostate cancer -what has gone wrong? A blueprint for the way forward in biomarker studies. Br J Cancer. 2015;112(1):140–148. doi: 10.1038/bjc.2014.588. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
