

When to incorporate point-of-care ultrasound (POCUS) into the initial assessment of acutely ill patients: a pilot crossover study to compare 2 POCUS-assisted simulation protocols
- PMID: 30200973
- PMCID: PMC6131841
- DOI: 10.1186/s12947-018-0132-0
When to incorporate point-of-care ultrasound (POCUS) into the initial assessment of acutely ill patients: a pilot crossover study to compare 2 POCUS-assisted simulation protocols
Abstract
Background: The purpose of this study was to determine the ideal timing for providers to perform point-of-care ultrasound (POCUS) with the least increase in workload.
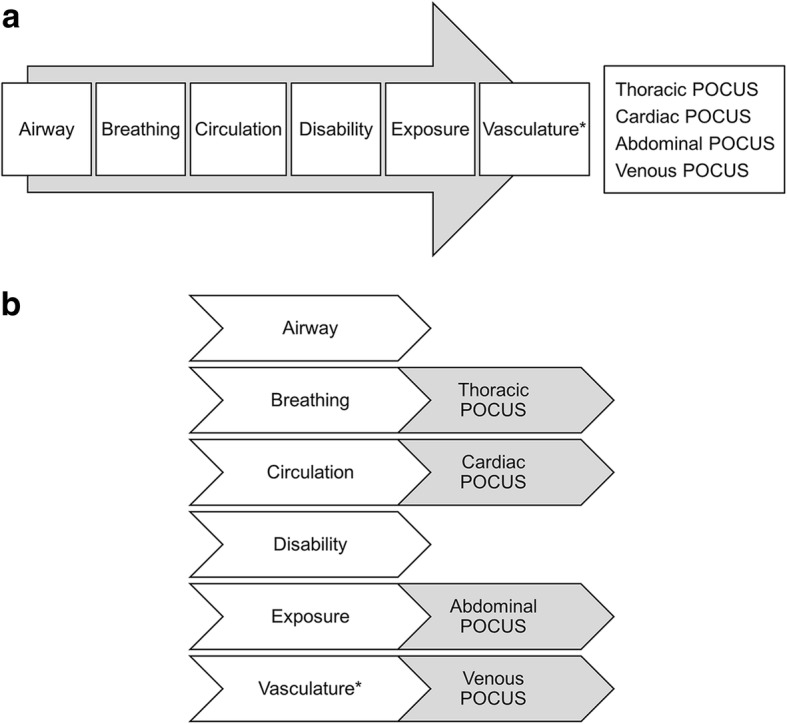
Methods: We conducted a pilot crossover study to compare 2 POCUS-assisted evaluation protocols for acutely ill patients: sequential (physical examination followed by POCUS) vs parallel (POCUS at the time of physical examination). Participants were randomly assigned to 2 groups according to which POCUS-assisted protocol (sequential vs parallel) was used during simulated scenarios. Subsequently, the groups were crossed over to complete assessment by using the other POCUS-assisted protocol in the same patient scenarios. Providers' workloads, measured with the National Aeronautics and Space Administration Task Load Index (NASA-TLX) and time to complete patient evaluation, were compared between the 2 protocols.
Results: Seven providers completed 14 assessments (7 sequential and 7 parallel). The median (IQR) total NASA-TLX score was 30 (30-50) in the sequential and 55 (50-65) in the parallel protocol (P = .03), which suggests a significantly lower workload in the sequential protocol. When individual components of the NASA-TLX score were evaluated, mental demand and frustration level were significantly lower in the sequential than in the parallel protocol (40 [IQR, 30-60] vs 50 [IQR, 40-70]; P = .03 and 25 [IQR, 20-35] vs 60 [IQR, 45-85]; P = .02, respectively). The time needed to complete the assessment was similar between the sequential and parallel protocols (8.7 [IQR, 6-9] minutes vs 10.1 [IQR, 7-11] minutes, respectively; P = .30).
Conclusions: A sequential POCUS-assisted protocol posed less workload to POCUS operators than the parallel protocol.
Keywords: Critical illness; Point-of-care; Simulation; Ultrasound.
Conflict of interest statement
Ethics approval and consent to participate
The study was approved by the Mayo Clinic Institutional Review Board (12–007998).
Consent for publication
Not applicable.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
-
- Ferrada P, Vanguri P, Anand RJ, Whelan J, Duane T, Aboutanos M, Malhotra A, Ivatury R. A, B, C, D, echo: limited transthoracic echocardiogram is a useful tool to guide therapy for hypotension in the trauma bay--a pilot study. J Trauma Acute Care Surg. 2013;74(1):220–223. doi: 10.1097/TA.0b013e318278918a. - DOI - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
