

Risk factors for damage in childhood-onset systemic lupus erythematosus in Asians: a case control study
- PMID: 30201026
- PMCID: PMC6131800
- DOI: 10.1186/s12969-018-0271-8
Risk factors for damage in childhood-onset systemic lupus erythematosus in Asians: a case control study
Abstract
Background: Accumulated damage is an important prognostic factor in systemic lupus erythematous. However, the pattern of disease damage and its risk factors have not been well studied in childhood-onset systemic lupus erythematosus (cSLE) in Asia. The objectives are to evaluate the pattern of damage and to identify the risk factors for accumulated damage in an Asian group of cSLE.
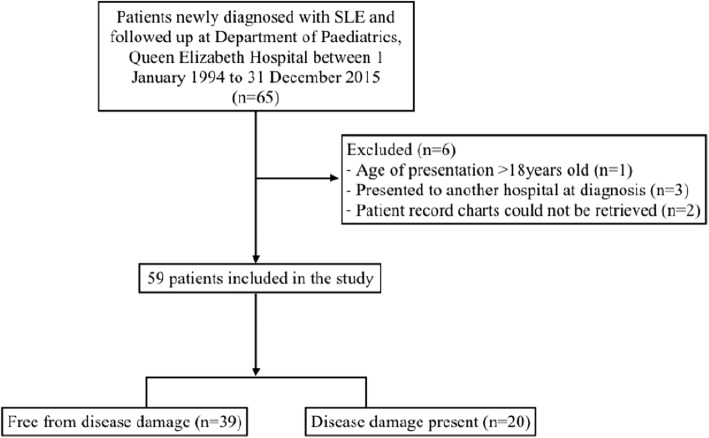
Methods: A retrospective chart review was conducted on a group of 59 patients with cSLE. Patient demographics and clinical variables were first collected at diagnosis. Over the course of their disease, clinical variables considered as risk factors for damage were also collected. Damage was measured using the Systemic Lupus International Collaborating Clinics/ American College of Rheumatology Damage Index (SDI) for each patient at their last encounter. Based on their SDI scores, patients were then dichotomized to two groups: a group with presence of disease damage (SDI ≥1) and a group with absence of disease damage (SDI score = 0). Clinical variables including age at diagnosis, gender, ethnicity, disease duration, disease manifestations, laboratory values at diagnosis, disease activity at diagnosis and last encounter, major organ involvement, number of lupus flares, major infection, and intensity of immunosuppressive medications were compared between the two groups. Growth failure and estimated glomerular filtration rate (eGFR) were also analysed as secondary outcomes.
Results: After a median disease duration and follow up of 7.8 years, 39 patients (66.1%) had no disease damage while 20 patients (33.9%) had acquired disease damage. Disease damage most frequently occurred in the ocular (15.3%), neuropsychiatric (11.9%) and musculoskeletal (11.9%) domains. The most frequent forms of damage were cataracts (11.9%), and avascular necrosis (unilateral and bilateral combined 10.2%). After controlling for other variables, presence of neuropsychiatric manifestations remained the only statistically significant risk factor for damage. The rate of growth failure in our group of patients was 16%. Patients who experienced growth failure were significantly younger at disease diagnosis. The median age of diagnosis was 10 for those who experienced growth failure, whereas the median age of diagnosis was 13 for those who did not experience growth failure. Despite a high rate of renal involvement in the group (79.7%), renal damage was only seen in 3.2% of the patients. 91.5% of the studied group had normal eGFR of ≥90 ml/min/1.73m2 at their last follow up.
Conclusion: This group of patients had a low rate of damage accrual, with one of the lowest rates in renal damage when compared to other cohorts reported. The presence of neuropsychiatric manifestations was identified as the most significant risk factor for disease damage, while the most frequent forms of damage were cataracts and avascular necrosis, which were both related to prolonged steroid use. Despite the limitations of this study, it highlights the need for larger prospective studies to understand the relationship between childhood-onset SLE and its resulting damage.
Keywords: Damage index; Outcome; Paediatrics; Systemic lupus erythematosus.
Conflict of interest statement
Ethics approval and consent to participate
This study was approved by the Research Ethics Committee of Kowloon Central/ Kowloon East cluster, Hong Kong (Reference number: KC/KE-16-0218/ER-1).
Consent for publication
No individual person’s data was presented in this study.
Competing interests
The authors declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

Similar articles
-
Dissecting the damage in Northern Greek patients with childhood-onset systemic lupus erythematosus: a retrospective cohort study.Rheumatol Int. 2015 Jul;35(7):1225-32. doi: 10.1007/s00296-014-3209-6. Epub 2015 Jan 14. Rheumatol Int. 2015. PMID: 25586653
-
The new 2019-EULAR/ACR classification criteria specific domains at diagnosis can predict damage accrual in 670 childhood-onset systemic lupus erythematosus patients.Lupus. 2021 Dec;30(14):2286-2291. doi: 10.1177/09612033211054397. Epub 2021 Oct 25. Lupus. 2021. PMID: 34689652
-
Assessment of clinical manifestations, disease activity and organ damage in 996 Korean patients with systemic lupus erythematosus: comparison with other Asian populations.Int J Rheum Dis. 2015 Feb;18(2):117-28. doi: 10.1111/1756-185X.12462. Epub 2014 Dec 19. Int J Rheum Dis. 2015. PMID: 25524656
-
Childhood Systemic Lupus Erythematosus: Presentation, management and long-term outcomes in an Australian cohort.Lupus. 2022 Feb;31(2):246-255. doi: 10.1177/09612033211069765. Epub 2022 Jan 16. Lupus. 2022. PMID: 35037500 Review.
-
Measuring Disease Damage and Its Severity in Childhood-Onset Systemic Lupus Erythematosus.Arthritis Care Res (Hoboken). 2018 Nov;70(11):1621-1629. doi: 10.1002/acr.23531. Arthritis Care Res (Hoboken). 2018. PMID: 29409150
Cited by
-
Musculoskeletal manifestations in childhood-onset systemic lupus erythematosus: an in-depth exploration.Ital J Pediatr. 2024 Aug 16;50(1):149. doi: 10.1186/s13052-024-01725-7. Ital J Pediatr. 2024. PMID: 39152510 Free PMC article.
-
Long-term growth and final adult height outcome in childhood-onset systemic lupus erythematosus.Pediatr Rheumatol Online J. 2022 Jan 24;20(1):4. doi: 10.1186/s12969-022-00663-0. Pediatr Rheumatol Online J. 2022. PMID: 35073942 Free PMC article.
-
Avascular necrosis in pediatric rheumatic diseases: an Italian retrospective multicentre study.Ital J Pediatr. 2025 Jan 29;51(1):20. doi: 10.1186/s13052-025-01845-8. Ital J Pediatr. 2025. PMID: 39876000 Free PMC article.
-
Epidemiology and risk factors for avascular necrosis in childhood systemic lupus erythematosus in a Taiwanese population.Sci Rep. 2020 Sep 23;10(1):15563. doi: 10.1038/s41598-020-71923-w. Sci Rep. 2020. PMID: 32968109 Free PMC article.
-
Long-Term Outcomes of Children and Adolescents With Biopsy-Proven Childhood-Onset Lupus Nephritis.Kidney Int Rep. 2022 Oct 21;8(1):141-150. doi: 10.1016/j.ekir.2022.10.014. eCollection 2023 Jan. Kidney Int Rep. 2022. PMID: 36644360 Free PMC article.
References
-
- Miettunen PM, et al. Gender and ethnic origin have no effect on longterm outcome of childhood-onset systemic lupus erythematosus. J Rheumatol. 2004;31(8):1650–1654. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
