

Effect of a combined brief narrative exposure therapy with case management versus treatment as usual in primary care for patients with traumatic stress sequelae following intensive care medicine: study protocol for a multicenter randomized controlled trial (PICTURE)
- PMID: 30201053
- PMCID: PMC6131807
- DOI: 10.1186/s13063-018-2853-7
Effect of a combined brief narrative exposure therapy with case management versus treatment as usual in primary care for patients with traumatic stress sequelae following intensive care medicine: study protocol for a multicenter randomized controlled trial (PICTURE)
Abstract
Background: Traumatic events like critical illness and intensive care are threats to life and bodily integrity and pose a risk factor for posttraumatic stress disorder (PTSD). PTSD affects the quality of life and morbidity and may increase health-care costs. Limited access to specialist care results in PTSD patients being treated in primary care settings. Narrative exposure therapy (NET) is based on the principles of cognitive behavioral therapy and has shown positive effects when delivered by health-care professionals other than psychologists. The primary aims of the PICTURE trial (from "PTSD after ICU survival") are to investigate the effectiveness and applicability of NET adapted for primary care with case management in adults diagnosed with PTSD after intensive care.
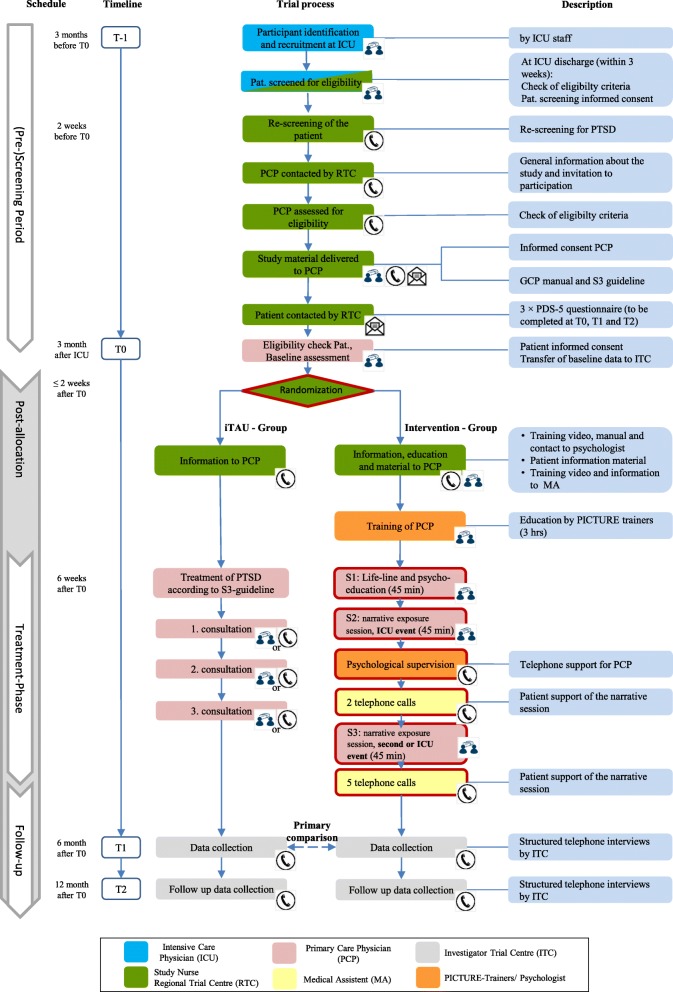
Methods/design: This is an investigator-initiated, multi-center, primary care-based, randomized controlled two-arm parallel group, observer-blinded superiority trial conducted throughout Germany. In total, 340 adult patients with a total score of at least 20 points on the posttraumatic diagnostic scale (PDS-5) 3 months after receiving intensive care treatment will be equally randomized to two groups: NET combined with case management and improved treatment as usual (iTAU). All primary care physicians (PCPs) involved will be instructed in the diagnosis and treatment of PTSD according to current German guidelines. PCPs in the iTAU group will deliver usual care during three consultations. In the experimental group, PCPs will additionally be trained to deliver an adapted version of NET (three sessions) supported by phone-based case management by a medical assistant. At 6 and 12 months after randomization, structured blinded telephone interviews will assess patient-reported outcomes. The primary composite endpoint is the absolute change from baseline at month 6 in PTSD symptom severity measured by the PDS-5 total score, which also incorporates the death of any study patients. Secondary outcomes cover the domains depression, anxiety, disability, health-related quality-of-life, and cost-effectiveness. The principal analysis is by intention to treat.
Discussion: If the superiority of the experimental intervention over usual care can be demonstrated, the combination of brief NET and case management could be a treatment option to relieve PTSD-related symptoms and to improve primary care after intensive care.
Trial registration: ClinicalTrials.gov, NCT03315390 . Registered on 10 October 2017. German Clinical Trials Register, DRKS00012589 . Registered on 17 October 2017.
Keywords: Intensive care (MeSH); Non-pharmacological (NON-Mesh); Primary health care (MeSH); Randomized controlled trial (MeSH); Stress disorders (MeSH).
Conflict of interest statement
Ethics approval and consent to participate
The screening and enrolment of participants did not start until the written and unrestricted positive vote of the local ethics committee was obtained. The ethics committee of the Medical Faculty of LMU Munich, Germany, approved the study protocol on 20 September 2017 (approval number 17–436) covering all participating sites. Modifications to the protocol will be submitted to the ethics committee for review. Written informed consent will be obtained from all participating patients and PCPs in the trial.
Consent for publication
Consent forms for the trial include consent for publication of results in peer-reviewed journals.
Competing interests
All authors have completed the uniform disclosure form of the International Committee of Medical Journal Editors at
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Steenbergen S, Rijkenberg S, Adonis T, Kroeze G, van Stijn I, Endeman H. Long-term treated intensive care patients outcomes: the one-year mortality rate, quality of life, health care use and long-term complications as reported by general practitioners. BMC Anesthesiol. 2015;15:142. doi: 10.1186/s12871-015-0121-x. - DOI - PMC - PubMed
-
- Maercker A, et al. ICD-11 Prevalence Rates of Posttraumatic Stress Disorder and Complex Posttraumatic Stress Disorder in a German Nationwide Sample. J Nerv Ment Dis. 2018;206(4):270-276. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
