

Exercise ventilatory inefficiency in heart failure and chronic obstructive pulmonary disease
- PMID: 30201380
- PMCID: PMC6242758
- DOI: 10.1016/j.ijcard.2018.09.007
Exercise ventilatory inefficiency in heart failure and chronic obstructive pulmonary disease
Abstract
Background: Dyspnea on exertion is common to both heart failure (HF) and chronic obstructive pulmonary disease (COPD), and it is important to discriminate whether symptoms are caused by HF or COPD in clinical practice. The ventilatory equivalent for carbon dioxide (V̇E/V̇CO2) slope and V̇E intercept (a reflection of pulmonary dead space) are two candidate non-invasive indices that could be used for this purpose. Thus, we compared non-invasive indexes of ventilatory efficiency in patients with HF and preserved or reduced ejection fraction (HFpEF and HFrEF, respectively) or COPD.
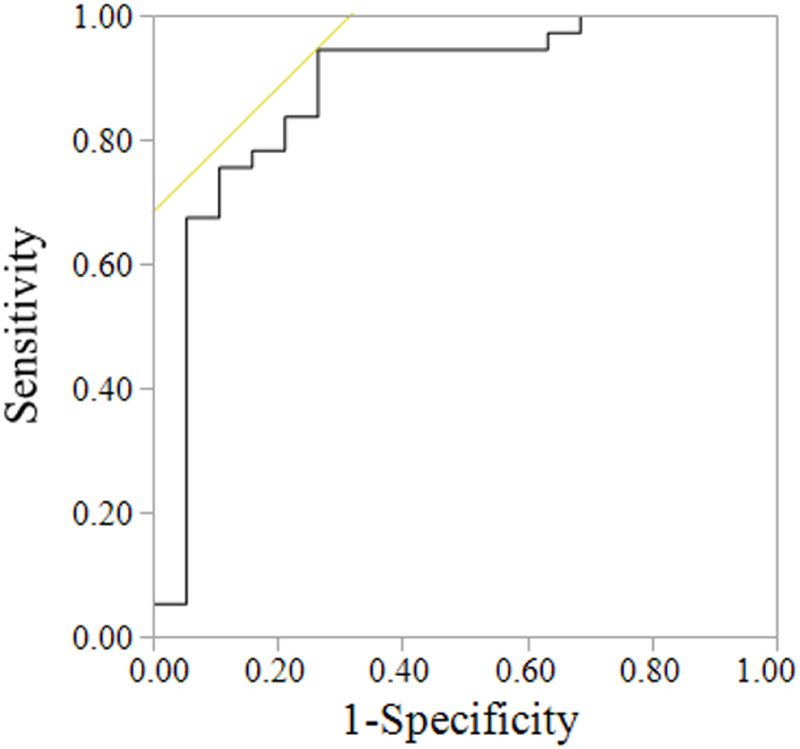
Methods: Patients with HFpEF (n = 21), HFrEF (n = 20), and COPD (n = 22) patients performed cardiopulmonary exercise testing to volitional fatigue. V̇E and gas exchange were measured via breath-by-breath open circuit spirometry. All data from rest to peak exercise were used to calculate V̇E/V̇CO2 slope and V̇E intercept using linear regression. Receiver operating characteristic (ROC) curves were constructed to determine optimized cutoffs for V̇E/V̇CO2 slope and V̇E intercept to discriminate HFpEF and HFrEF from COPD.
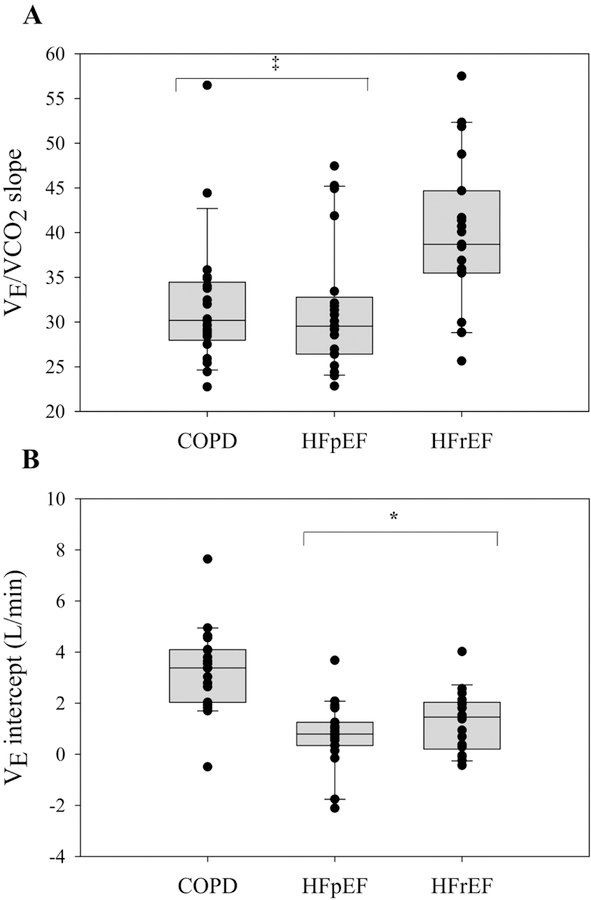
Results: HFrEF patients had a greater V̇E/V̇CO2 slope than HFpEF and COPD patients (HFrEF: 40 ± 9; HFpEF: 32 ± 7; COPD: 32 ± 7) (p < 0.01). COPD patients had a greater V̇E intercept than HFpEF and HFrEF patients (COPD: 3.32 ± 1.66; HFpEF: 0.77 ± 1.23; HFrEF: 1.28 ± 1.19 L/min) (p < 0.01). A V̇E intercept of 2.64 L/min discriminated COPD from HF patients (AUC: 0.88, p < 0.01), while V̇E/V̇CO2 slope did not (p = 0.11).
Conclusion: These findings demonstrate that V̇E intercept, not V̇E/V̇CO2 slope, may discriminate COPD from both HFpEF and HFrEF patients.
Keywords: Breathing strategy; Diastolic heart failure; Systolic heart failure; V(E)/VCO(2) slope; Ventilatory intercept.
Copyright © 2018 Elsevier B.V. All rights reserved.
Conflict of interest statement
Figures
Similar articles
-
Physiological dead space and arterial carbon dioxide contributions to exercise ventilatory inefficiency in patients with reduced or preserved ejection fraction heart failure.Eur J Heart Fail. 2017 Dec;19(12):1675-1685. doi: 10.1002/ejhf.913. Epub 2017 Oct 8. Eur J Heart Fail. 2017. PMID: 28990307 Free PMC article.
-
Ventilatory response to carbon dioxide output in subjects with congestive heart failure and in patients with COPD with comparable exercise capacity.Respir Care. 2014 Jul;59(7):1034-41. doi: 10.4187/respcare.02629. Epub 2013 Sep 17. Respir Care. 2014. PMID: 24046458
-
Impact of chronic obstructive pulmonary disease on exercise ventilatory efficiency in heart failure.Int J Cardiol. 2015;189:134-40. doi: 10.1016/j.ijcard.2015.03.422. Epub 2015 Mar 31. Int J Cardiol. 2015. PMID: 25889444
-
Effect of Aerobic Exercise on Peak Oxygen Consumption, VE/VCO2 Slope, and Health-Related Quality of Life in Patients with Heart Failure with Preserved Left Ventricular Ejection Fraction: a Systematic Review and Meta-Analysis.Curr Atheroscler Rep. 2019 Nov 9;21(11):45. doi: 10.1007/s11883-019-0806-6. Curr Atheroscler Rep. 2019. PMID: 31707525
-
Chronic Obstructive Pulmonary Disease in Heart Failure: Challenges in Diagnosis and Treatment for HFpEF and HFrEF.Curr Heart Fail Rep. 2024 Jun;21(3):163-173. doi: 10.1007/s11897-024-00660-2. Epub 2024 Mar 28. Curr Heart Fail Rep. 2024. PMID: 38546964 Review.
Cited by
-
Ventilatory limitations in patients with HFpEF and obesity.Respir Physiol Neurobiol. 2023 Dec;318:104167. doi: 10.1016/j.resp.2023.104167. Epub 2023 Sep 26. Respir Physiol Neurobiol. 2023. PMID: 37758032 Free PMC article.
-
Higher Work of Breathing During Exercise in Heart Failure With Preserved Ejection Fraction.Chest. 2023 Jun;163(6):1492-1505. doi: 10.1016/j.chest.2022.11.039. Epub 2022 Dec 5. Chest. 2023. PMID: 36470415 Free PMC article.
-
Exertional ventilation/carbon dioxide output relationship in COPD: from physiological mechanisms to clinical applications.Eur Respir Rev. 2021 Sep 15;30(161):200190. doi: 10.1183/16000617.0190-2020. Print 2021 Sep 30. Eur Respir Rev. 2021. PMID: 34526312 Free PMC article. Review.
-
Physical Activity Intolerance and Cardiorespiratory Dysfunction in Patients with Moderate-to-Severe Traumatic Brain Injury.Sports Med. 2019 Aug;49(8):1183-1198. doi: 10.1007/s40279-019-01122-9. Sports Med. 2019. PMID: 31098990 Review.
-
Measurement and Interpretation of Exercise Ventilatory Efficiency.Front Physiol. 2020 Jun 25;11:659. doi: 10.3389/fphys.2020.00659. eCollection 2020. Front Physiol. 2020. PMID: 32714201 Free PMC article. Review.
References
-
- Hawkins NM, Virani S, Ceconi C. Heart failure and chronic obstructive pulmonary disease: the challenges facing physicians and health services. Eur Heart J 2013. September;34(36):2795–2803. - PubMed
-
- Guazzi M, Myers J, Arena R. Cardiopulmonary exercise testing in the clinical and prognostic assessment of diastolic heart failure. J Am Coll Cardiol 2005. November 15;46(10):1883–1890. - PubMed
-
- Arena R, Humphrey R. Comparison of ventilatory expired gas parameters used to predict hospitalization in patients with heart failure. Am Heart J 2002. March;143(3):427–432. - PubMed
-
- Guazzi M, Reina G, Tumminello G, Guazzi MD. Exercise ventilation inefficiency and cardiovascular mortality in heart failure: the critical independent prognostic value of the arterial CO2 partial pressure. Eur Heart J 2005. March;26(5):472–480. - PubMed
-
- Thirapatarapong W, Armstrong HF, Thomashow BM, Bartels MN. Differences in gas exchange between severities of chronic obstructive pulmonary disease. Respir Physiol Neurobiol 2013. March 01;186(1):81–86. - PubMed
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
