

Susceptible period for cardiovascular complications in patients recovering from sepsis
- PMID: 30201613
- PMCID: PMC6131076
- DOI: 10.1503/cmaj.171284
Susceptible period for cardiovascular complications in patients recovering from sepsis
Abstract
Background: Patients are at increased risk of cardiovascular complications while recovering from sepsis. We aimed to study the temporal change and susceptible periods for cardiovascular complications in patients recovering from sepsis by using a national database.
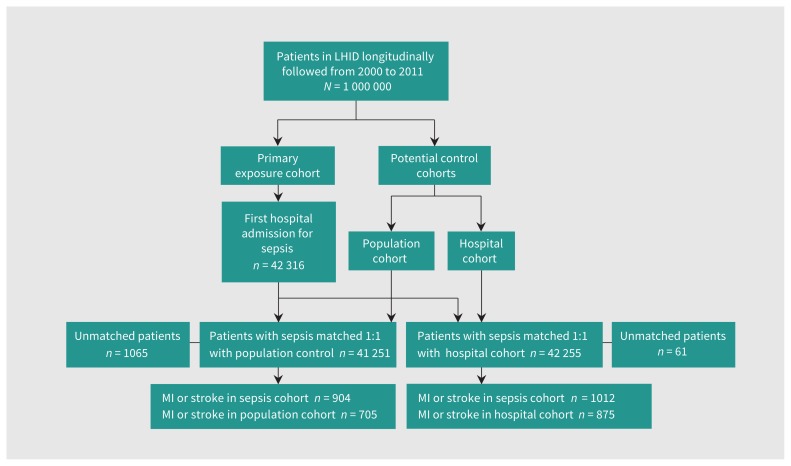
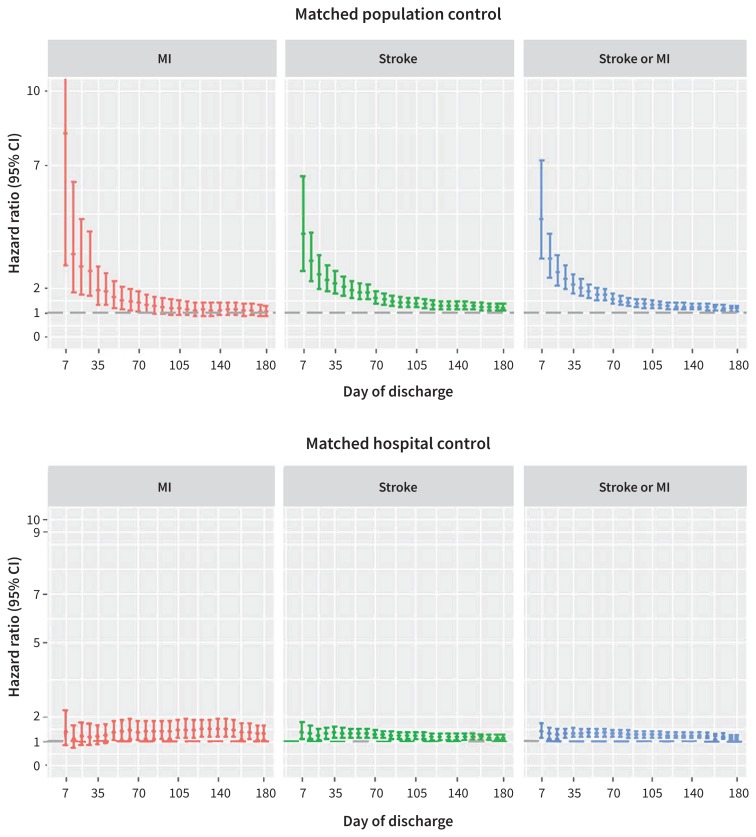
Methods: In this retrospective population-based cohort study, patients with sepsis were identified from the National Health Insurance Research Database in Taiwan. We estimated the risk of myocardial infarction (MI) and stroke following sepsis by comparing a sepsis cohort to a matched population and hospital control cohort. The primary outcome was first occurrence of MI or stroke requiring admission to hospital during the 180-day period following discharge from hospital after sepsis. To delineate the risk profile over time, we plotted the weekly risk of MI and stroke against time using the Cox proportional hazards model. We determined the susceptible period by fitting the 2 phases of time-dependent risk curves with free-knot splines, which highlights the turning point of the risk of MI and stroke after discharge from the hospital.
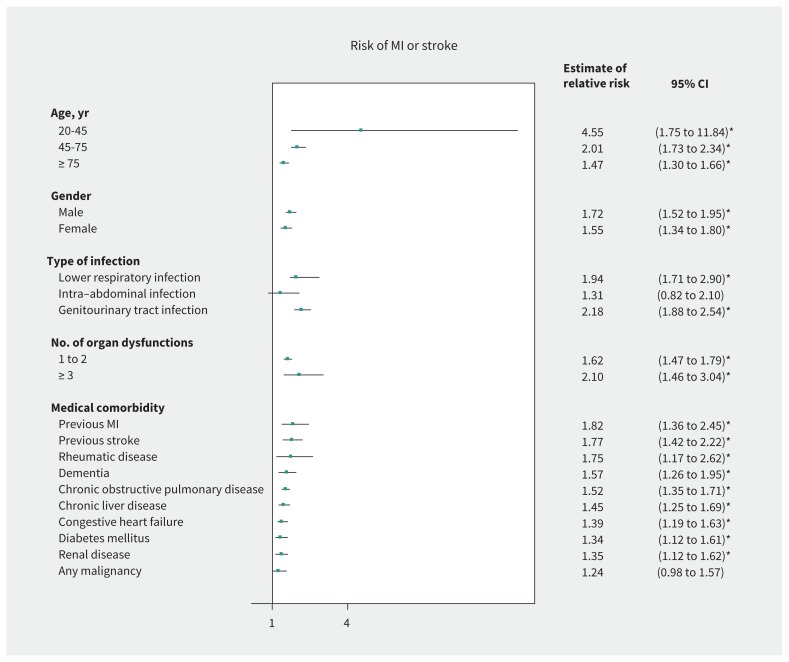
Results: We included 42 316 patients with sepsis; stroke developed in 831 of these patients and MI developed in 184 within 180 days of discharge from hospital. Compared with population controls, patients recovering from sepsis had the highest risk for MI or stroke in the first week after discharge (hazard ratio [HR] 4.78, 95% confidence interval [CI] 3.19 to 7.17; risk difference 0.0028, 95% CI 0.0021 to 0.0034), with the risk decreasing rapidly until the 28th day (HR 2.38, 95% CI 1.94 to 2.92; risk difference 0.0045, 95% CI 0.0035 to 0.0056) when the risk stabilized. In a repeated analysis comparing the sepsis cohort with the nonsepsis hospital control cohort, we found an attenuated but still marked elevated risk before day 36 after discharge (HR 1.32, 95% CI 1.15 to 1.52; risk difference 0.0026, 95% CI 0.0013 to 0.0039). The risk of MI or stroke was found to interact with age, with younger patients being associated with a higher risk than older patients (interaction p = 0.0004).
Interpretation: Compared with the general population with similar characteristics, patients recovering from sepsis had a markedly elevated risk of MI or stroke in the first 4 weeks after discharge from hospital. More close monitoring and pharmacologic prevention may be required for these patients at the specified time.
© 2018 Joule Inc. or its licensors.
Conflict of interest statement
Competing interests: None declared.
Figures
Similar articles
-
Impact of post-sepsis cardiovascular complications on mortality in sepsis survivors: a population-based study.Crit Care. 2019 Sep 2;23(1):293. doi: 10.1186/s13054-019-2579-2. Crit Care. 2019. PMID: 31477181 Free PMC article.
-
Risk Factors for Myocardial Infarction and Stroke Among Sepsis Survivors: A Competing Risks Analysis.J Intensive Care Med. 2020 Jan;35(1):34-41. doi: 10.1177/0885066619844936. Epub 2019 May 12. J Intensive Care Med. 2020. PMID: 31079522
-
Renal complications and subsequent mortality in acute critically ill patients without pre-existing renal disease.CMAJ. 2018 Sep 10;190(36):E1070-E1080. doi: 10.1503/cmaj.171382. CMAJ. 2018. PMID: 30201614 Free PMC article.
-
Risk of type 2 diabetes mellitus in patients with acute critical illness: a population-based cohort study.Intensive Care Med. 2016 Jan;42(1):38-45. doi: 10.1007/s00134-015-4044-2. Epub 2015 Sep 14. Intensive Care Med. 2016. PMID: 26370689
-
Depression, stroke, and dementia in patients with myocardial infarction.Dan Med J. 2018 Apr;65(4):B5423. Dan Med J. 2018. PMID: 29619929 Review.
Cited by
-
Divergent Sepsis Pathophysiology in Older Adults.Antioxid Redox Signal. 2021 Dec;35(16):1358-1375. doi: 10.1089/ars.2021.0056. Epub 2021 Oct 1. Antioxid Redox Signal. 2021. PMID: 34210173 Free PMC article. Review.
-
Parallel Dysregulated Immune Response in Severe Forms of COVID-19 and Bacterial Sepsis via Single-Cell Transcriptome Sequencing.Biomedicines. 2023 Mar 3;11(3):778. doi: 10.3390/biomedicines11030778. Biomedicines. 2023. PMID: 36979757 Free PMC article.
-
Gasdermin D Mediates Inflammation-Induced Defects in Reverse Cholesterol Transport and Promotes Atherosclerosis.Front Cell Dev Biol. 2021 Jul 28;9:715211. doi: 10.3389/fcell.2021.715211. eCollection 2021. Front Cell Dev Biol. 2021. PMID: 34395445 Free PMC article.
-
Association between sepsis survivorship and long-term cardiovascular outcomes in adults: a systematic review and meta-analysis.Intensive Care Med. 2021 Sep;47(9):931-942. doi: 10.1007/s00134-021-06479-y. Epub 2021 Aug 9. Intensive Care Med. 2021. PMID: 34373953
-
Long-term risk and predictors of cerebrovascular events following sepsis hospitalization: A systematic review and meta-analysis.Front Med (Lausanne). 2022 Nov 25;9:1065476. doi: 10.3389/fmed.2022.1065476. eCollection 2022. Front Med (Lausanne). 2022. PMID: 36507522 Free PMC article.
References
-
- Navaneelan T, Alam S, Peters P, et al. Deaths involving sepsis in Canada. Ottawa: Statistics Canada; 2016. Cat no 82-624-X201600114308.
-
- Ou SM, Chu H, Chao PW, et al. Long-term mortality and major adverse cardiovascular events in sepsis survivors: a nationwide population-based study. Am J Respir Crit Care Med 2016;194:209–17. - PubMed
-
- Merx MW, Weber C. Sepsis and the heart. Circulation 2007;116:793–802. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical