

Review
doi: 10.1101/cshperspect.a030627.
Immunotherapy for Prostate Cancer
Affiliations
- PMID: 30201787
- PMCID: PMC6496329
- DOI: 10.1101/cshperspect.a030627
Item in Clipboard
Review
Immunotherapy for Prostate Cancer
Cold Spring Harb Perspect Med.
.
Abstract
Immunotherapy with agents that block immune checkpoints is a mainstay of therapy for several common tumor types; so far, prostate cancer is not among those treated using this method. The observed lack of activity in prostate cancer is not due to a lack of testing; several agents have been evaluated both alone and in combination. Although several combination strategies show some promise, it appears likely that a greater understanding of the prostate cancer tumor microenvironment and baseline immune response will be required to optimize future treatment strategies.
Copyright © 2019 Cold Spring Harbor Laboratory Press; all rights reserved.
Figures
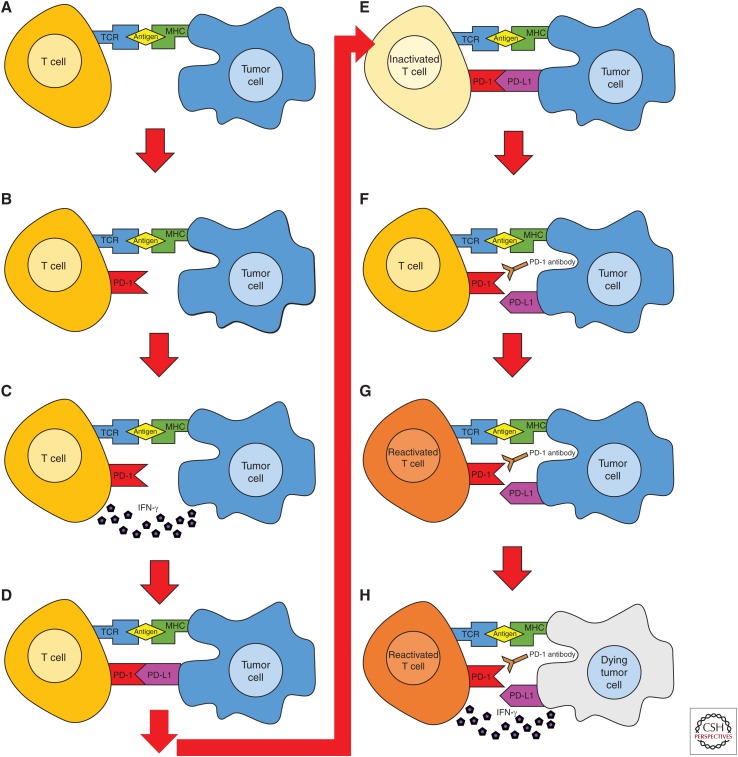
Adaptive immune resistance and reinvigoration of antitumor immunity by programmed death-1 (PD-1) blockade. (A–H) PD-1 is up-regulated by antigen recognition, leading to secretion of the effector cytokine interferon (IFN)-γ. Sensing of IFN-γ by tumor cells results in up-regulation of PD-L1, which binds to PD-1 on the effector T cell, strongly inhibiting T-cell effector function and adaptive immunity. PD-1 blockade inhibits this negative interaction, leading to reacquisition of T-cell effector function and tumor lysis.
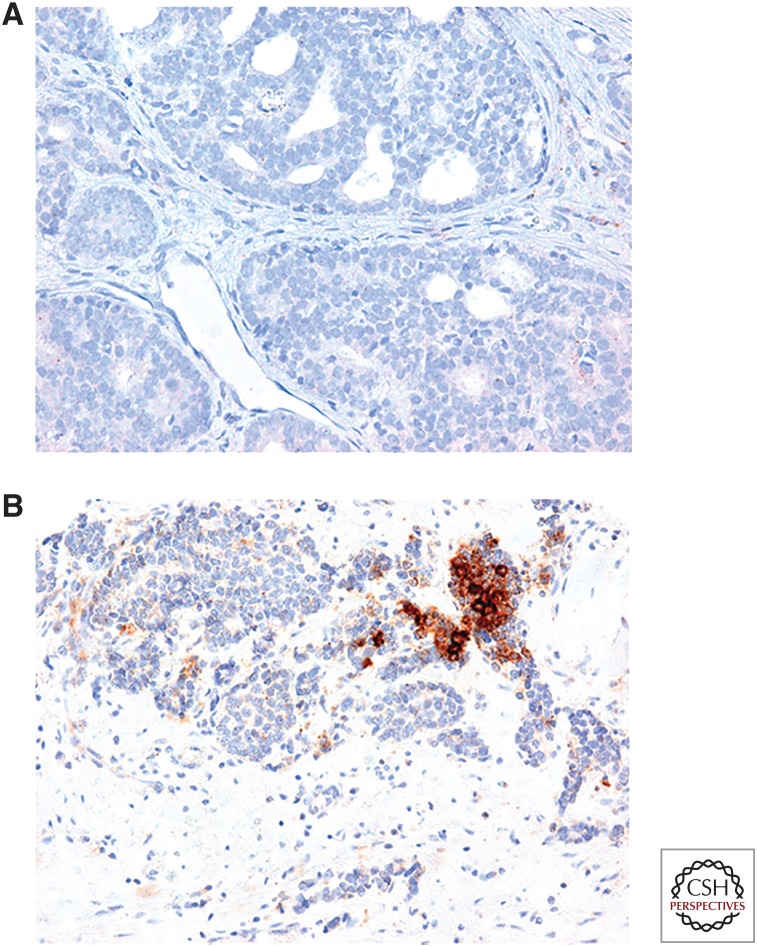
Ligand for programmed death-1 (PD-L1) expression in metastatic prostate cancer. (A,B) Immunohistochemistry for PD-L1 in metastatic prostate cancer lesions. The majority of stained lesions are completely PD-L1-negative (A); ∼30% stain positive for PD-L1. (Images courtesy of M. Haffner, Johns Hopkins University.)
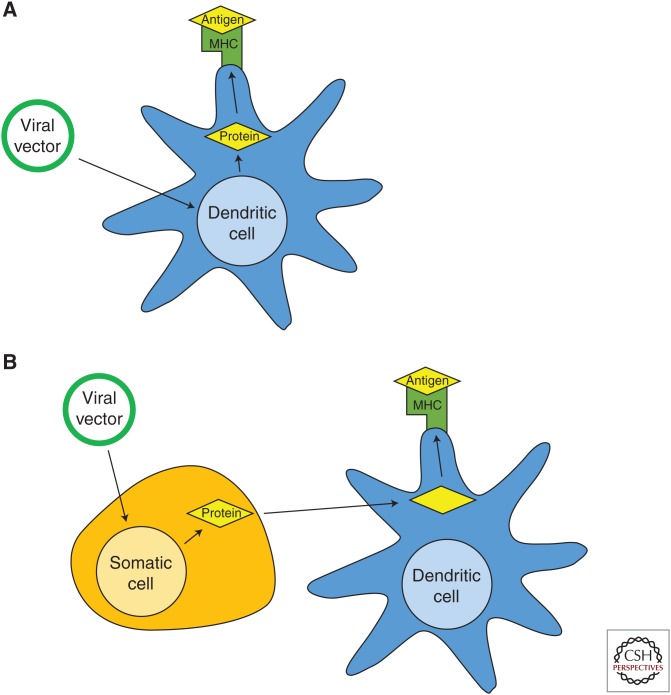
Direct and cross-presentation of vaccine-encoded antigens. (A) Direct presentation. The vector directly infects antigen-presenting cell, leading to processing and presentation of tumor antigen on class I major histocompatibility complex (MHC). (B) Cross-presentation. The vector infects epithelial cells, leading to lysis. Cellular debris is taken up by nearby antigen presenting cells, processed, and presented on class I MHC.
References
-
- Agata Y, Kawasaki A, Nishimura H, Ishida Y, Tsubata T, Yagita H, Honjo T. 1996. Expression of the PD-1 antigen on the surface of stimulated mouse T and B lymphocytes. Int Immunol 8: 765–772. - PubMed
-
- Arlen PM, Gulley JL, Madan RA, Hodge JW, Schlom J. 2007. Preclinical and clinical studies of recombinant poxvirus vaccines for carcinoma therapy. Crit Rev Immunol 27: 451–462. - PubMed
-
- Beer TM, Kwon ED, Drake CG, Fizazi K, Logothetis C, Gravis G, Ganju V, Polikoff J, Saad F, Humanski P, et al. 2017. Randomized, double-blind, phase III trial of ipilimumab versus placebo in asymptomatic or minimally symptomatic patients with metastatic chemotherapy-naive castration-resistant prostate cancer. J Clin Oncol 35: 40–47. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical