

Real-world retrospective cohort study ARCTIC shows burden of comorbidities in Swedish COPD versus non-COPD patients
- PMID: 30202023
- PMCID: PMC6131165
- DOI: 10.1038/s41533-018-0101-y
Real-world retrospective cohort study ARCTIC shows burden of comorbidities in Swedish COPD versus non-COPD patients
Abstract
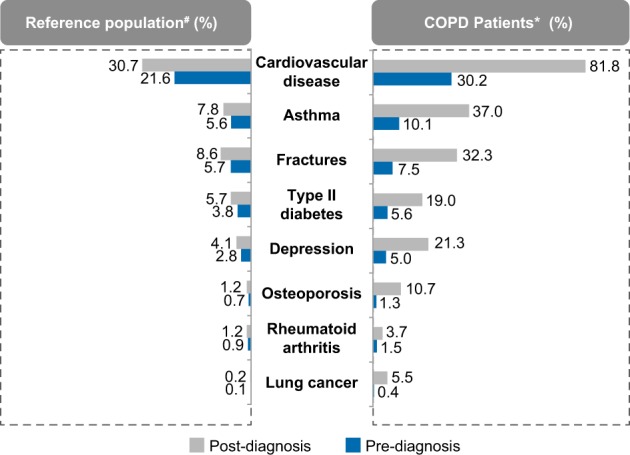
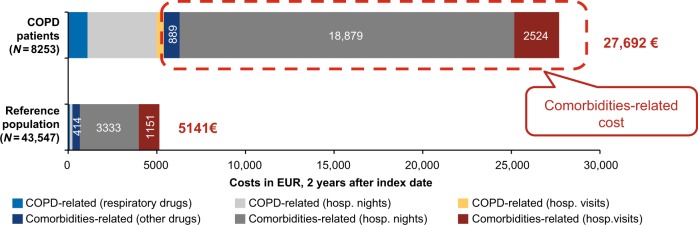
This study aimed to generate real-world evidence to assess the burden of comorbidities in COPD patients, to effectively manage these patients and optimize the associated healthcare resource allocation. ARCTIC is a large, real-world, retrospective cohort study conducted in Swedish COPD patients using electronic medical record data collected between 2000 and 2014. These patients were studied for prevalence of various comorbidities and for association of these comorbidities with exacerbations, mortality, and healthcare costs compared with an age-, sex-, and comorbidities-matched non-COPD reference population. A total of 17,479 patients with COPD were compared with 84,514 non-COPD reference population. A significantly higher prevalence of various comorbidities was observed in COPD patients 2 years post-diagnosis vs. reference population, with the highest percentage increase observed for cardiovascular diseases (81.8% vs. 30.7%). Among the selected comorbidities, lung cancer was relatively more prevalent in COPD patients vs. reference population (relative risk, RR = 5.97, p < 0.0001). Ischemic heart disease, hypertension, depression, anxiety, sleep disorders, osteoporosis, osteoarthritis, and asthma caused increased mortality rates in COPD patients. Comorbidities that were observed to be significantly associated with increased number of severe exacerbations in COPD patients included heart failure, ischemic heart disease, depression/anxiety, sleep disorders, osteoporosis, lung cancer, and stroke. The cumulative healthcare costs associated with comorbidities over 2 years after the index date were observed to be significantly higher in COPD patients (€27,692) vs. reference population (€5141) (p < 0.0001). The data support the need for patient-centered treatment strategies and targeted healthcare resource allocation to reduce the humanistic and economic burden associated with COPD comorbidities.
Conflict of interest statement
B.S. has received honoraria for educational activities and lectures from AstraZeneca, Boehringer Ingelheim, Meda, Novartis and Teva, and has served on advisory boards arranged by AstraZeneca, Novartis, Meda, GlaxoSmithKline, Teva and Boehringer Ingelheim. K.K., J.-B.G., and F.S.G. are employed by Novartis Pharma AG, Basel, Switzerland. C.J. has received honoraria for educational activities and lectures from Novartis, AstraZeneca, GlaxoSmithKline, TEVA and Boehringer Ingelheim outside the submitted work. G.J. has participated in the steering committee by Novartis for this study and served on advisory boards arranged by AstraZeneca, Novo Nordisk, and Takeda. K.L. has, during the last 5 years, on one or more occasion served in an advisory board and/or served as speaker and/or participated in education arranged by AstraZeneca, Boehringer Ingelheim, Chiesi, GlaxoSmithKline, Orion, Novartis, TEVA and Takeda. L.J. and M.U. are employed by IQVIA. K.L. has received payments for educational activities and lectures from AstraZeneca, GlaxoSmithKline, Meda, MSD, Novartis and Nycomed, served on advisory boards arranged by Novartis and Meda, and has participated in the steering committee by Novartis for this study.
Figures
Similar articles
-
Gender differences among Swedish COPD patients: results from the ARCTIC, a real-world retrospective cohort study.NPJ Prim Care Respir Med. 2019 Dec 10;29(1):45. doi: 10.1038/s41533-019-0157-3. NPJ Prim Care Respir Med. 2019. PMID: 31822681 Free PMC article.
-
Economic burden of COPD in a Swedish cohort: the ARCTIC study.Int J Chron Obstruct Pulmon Dis. 2018 Jan 11;13:275-285. doi: 10.2147/COPD.S149633. eCollection 2018. Int J Chron Obstruct Pulmon Dis. 2018. PMID: 29391785 Free PMC article.
-
Impact of COPD diagnosis timing on clinical and economic outcomes: the ARCTIC observational cohort study.Int J Chron Obstruct Pulmon Dis. 2019 May 13;14:995-1008. doi: 10.2147/COPD.S195382. eCollection 2019. Int J Chron Obstruct Pulmon Dis. 2019. PMID: 31190785 Free PMC article.
-
Burden of chronic obstructive pulmonary disease: healthcare costs and beyond.Allergy Asthma Proc. 2015 Jan-Feb;36(1):4-10. doi: 10.2500/aap.2015.36.3812. Allergy Asthma Proc. 2015. PMID: 25562549 Free PMC article. Review.
-
Chronic obstructive pulmonary disease: the disease and its burden to society.Proc Am Thorac Soc. 2006 Sep;3(7):619-23. doi: 10.1513/pats.200603-093SS. Proc Am Thorac Soc. 2006. PMID: 16963544 Review.
Cited by
-
Challenges and opportunities for telehealth in the management of chronic obstructive pulmonary disease: a qualitative case study in Greece.BMC Med Inform Decis Mak. 2020 Sep 10;20(1):216. doi: 10.1186/s12911-020-01221-y. BMC Med Inform Decis Mak. 2020. PMID: 32912224 Free PMC article.
-
Factors related to mortality in patients with chronic obstructive pulmonary disease in Colombian population.Biomedica. 2024 May 31;44(Sp. 1):151-159. doi: 10.7705/biomedica.7140. Biomedica. 2024. PMID: 39079138 Free PMC article. English, Spanish.
-
Impact of tobacco-related chronic obstructive pulmonary disease on developmental trajectories of comorbidities in the Taiwan population.Sci Rep. 2020 Dec 3;10(1):21025. doi: 10.1038/s41598-020-78325-y. Sci Rep. 2020. PMID: 33273701 Free PMC article.
-
COPD - do the right thing.BMC Fam Pract. 2021 Dec 11;22(1):244. doi: 10.1186/s12875-021-01583-w. BMC Fam Pract. 2021. PMID: 34895164 Free PMC article. Review.
-
Challenges to the Application of Integrated, Personalized Care for Patients with COPD-A Vision for the Role of Clinical Information.J Clin Med. 2020 May 2;9(5):1311. doi: 10.3390/jcm9051311. J Clin Med. 2020. PMID: 32370150 Free PMC article. Review.
References
-
- GOLD. Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease, http://goldcopd.org/ (2017).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
