

Clinical Effectiveness of Lifestyle Health Coaching: Case Study of an Evidence-Based Program
- PMID: 30202328
- PMCID: PMC6125027
- DOI: 10.1177/1559827615592351
Clinical Effectiveness of Lifestyle Health Coaching: Case Study of an Evidence-Based Program
Abstract
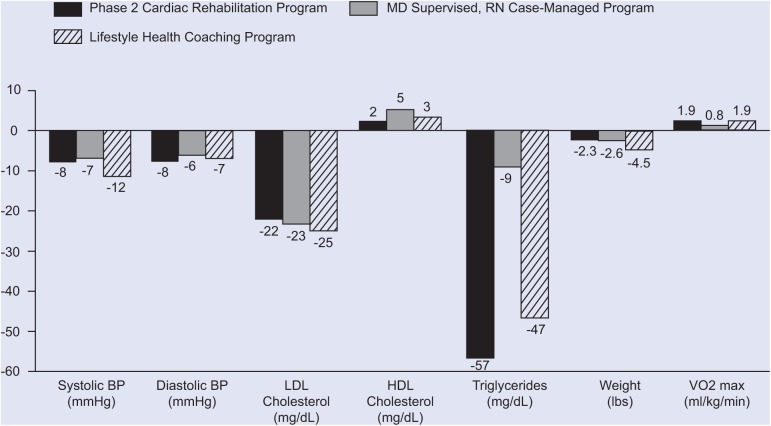
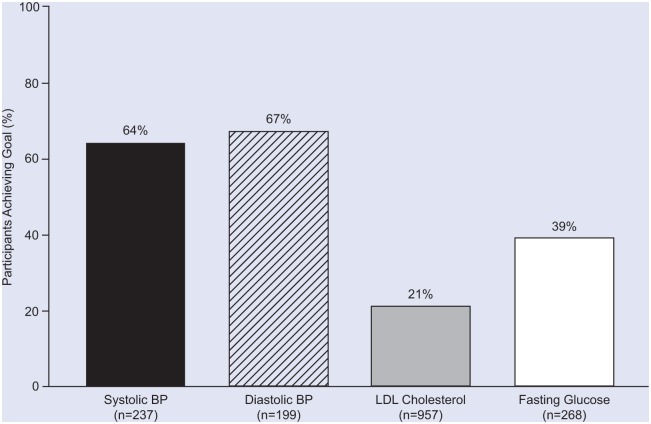
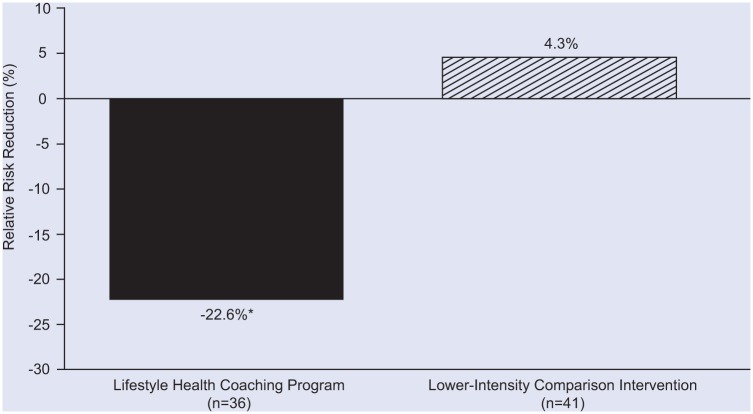
We have developed, tested, and successfully implemented an affordable, evidence-based, technology-enabled, data-driven, outcomes-oriented, comprehensive lifestyle health coaching (LHC) program. The LHC program has been used primarily to provide services to employees of larger employers (ie, with at least 3000 employees) but has also been implemented in a variety of other settings, including hospitals, cardiac rehabilitation centers, physician practices, and as part of multicenter clinical trials. The program is delivered mainly using the telephone and Internet. Health coaches are guided by a Web-based participant management and tracking system. Lifestyle management interventions are based on several behavior change models and strategies, especially adult learning theory, social learning theory, the stages of change model, single concept learning theory, and motivational interviewing. The program is administered by nonphysician health professionals whose services are integrated with the care provided by participants' physicians. Outcomes data from published studies, including randomized clinical trials and independent third-party conducted research, have documented the clinical effectiveness of this evidence-based approach in terms of modification of multiple risk factors in healthy persons as well as those with certain common chronic diseases.
Keywords: exercise; nutrition; prevention; wellness.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Dr. Gordon, Dr. Salmon, Dr. Wright, Mr. Faircloth and Mr. Reid are members of and Ms. Gordon is an employee of a population health management company (INTERVENT International, LLC).
Figures
Similar articles
-
Innovative approaches to comprehensive cardiovascular disease risk reduction in clinical and community-based settings.Curr Atheroscler Rep. 2001 Nov;3(6):498-506. doi: 10.1007/s11883-001-0040-9. Curr Atheroscler Rep. 2001. PMID: 11602070 Review.
-
The effectiveness of internet-based e-learning on clinician behavior and patient outcomes: a systematic review protocol.JBI Database System Rev Implement Rep. 2015 Jan;13(1):52-64. doi: 10.11124/jbisrir-2015-1919. JBI Database System Rev Implement Rep. 2015. PMID: 26447007
-
A Technology-Assisted Telephone Intervention for Work-Related Stress Management: Pilot Randomized Controlled Trial.J Med Internet Res. 2022 Jul 13;24(7):e26569. doi: 10.2196/26569. J Med Internet Res. 2022. PMID: 35830233 Free PMC article.
-
Effectiveness of programmes as part of primary prevention demonstrated on the example of cardiovascular diseases and the metabolic syndrome.GMS Health Technol Assess. 2011 Apr 1;7:Doc02. doi: 10.3205/hta000093. GMS Health Technol Assess. 2011. PMID: 21468290 Free PMC article.
-
A Systematic Review of the Literature on Health and Wellness Coaching: Defining a Key Behavioral intervention in Healthcare.Glob Adv Health Med. 2013 Jul;2(4):38-57. doi: 10.7453/gahmj.2013.042. Glob Adv Health Med. 2013. PMID: 24416684 Free PMC article. Review.
Cited by
-
An Evidence Based Rationale for Health and Wellness Coaching as a Complementary Certification in Undergraduate Health Education.Am J Lifestyle Med. 2023 Jul 12;18(2):181-185. doi: 10.1177/15598276231189206. eCollection 2024 Mar-Apr. Am J Lifestyle Med. 2023. PMID: 38559783 Free PMC article.
-
Lifestyle Modification for Secondary Stroke Prevention.Am J Lifestyle Med. 2016 Feb 21;12(2):140-147. doi: 10.1177/1559827616633683. eCollection 2018 Mar-Apr. Am J Lifestyle Med. 2016. PMID: 30202386 Free PMC article. Review.
-
Cost effectiveness of nonpharmacological prevention programs for diabetes: A systematic review of trial-based studies.Chronic Dis Transl Med. 2023 Aug 31;10(1):12-21. doi: 10.1002/cdt3.89. eCollection 2024 Mar. Chronic Dis Transl Med. 2023. PMID: 38450300 Free PMC article. Review.
-
Does Self-Perceived Diet Quality Align with Nutrient Intake? A Cross-Sectional Study Using the Food Nutrient Index and Diet Quality Score.Nutrients. 2023 Jun 12;15(12):2720. doi: 10.3390/nu15122720. Nutrients. 2023. PMID: 37375624 Free PMC article.
-
Preliminary Effectiveness Study of a Community-Based Wellness Coaching for Cancer Survivors Program.Am J Lifestyle Med. 2022 Mar 1;18(4):465-474. doi: 10.1177/15598276221076040. eCollection 2024 Jul-Aug. Am J Lifestyle Med. 2022. PMID: 39262887 Free PMC article. Review.
References
-
- Roberts CK, Barnard RJ. Effects of exercise and diet on chronic disease. J Appl Physiol. 2005;78:3-30. - PubMed
-
- Gordon NF. Clinical effectiveness of lifestyle management programs: importance of the class effect paradox. Curr Treat Options. 2013;15:675-680. - PubMed
-
- Mayosi BM, Flisher AJ, Lalloo UG, Sitas F, Tollman SM, Bradshaw D. The burden of non-communicable diseases in South Africa. Lancet. 2009;374:934-947. - PubMed
-
- American Heart Association. Preventing cancer, cardiovascular disease, and diabetes: a common agenda for the American Cancer Society, the American Diabetes Association, and the American Heart Association. Circulation. 2004;109:3244-3255. - PubMed
-
- Mozaffarian D, Benjamin EJ, Go AS, et al. Heart disease and stroke statistics—2015 update: a report from the American Heart Association. Circulation. 2015;131:e29-e322. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources