

Emergency Providers' Pain Management in Patients Transferred to Intensive Care Unit for Urgent Surgical Interventions
- PMID: 30202502
- PMCID: PMC6123091
- DOI: 10.5811/westjem.2018.7.37989
Emergency Providers' Pain Management in Patients Transferred to Intensive Care Unit for Urgent Surgical Interventions
Abstract
Introduction: Pain is the most common complaint for an emergency department (ED) visit, but ED pain management is poor. Reasons for poor pain management include providers' concerns for drug-seeking behaviors and perceptions of patients' complaints. Patients who had objective findings of long bone fractures were more likely to receive pain medication than those who did not, despite pain complaints. We hypothesized that patients who were interhospital-transferred from an ED to an intensive care unit (ICU) for urgent surgical interventions would display objective pathology for pain and thus receive adequate pain management at ED departure.
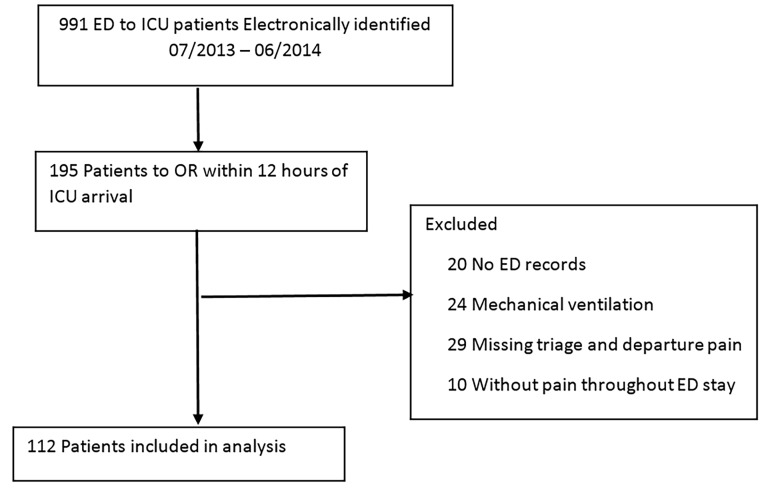
Methods: This was a retrospective study at a single, quaternary referral, academic medical center. We included non-trauma adult ED patients who were interhospital-transferred and underwent operative interventions within 12 hours of ICU arrival between July 2013 and June 2014. Patients who had incomplete ED records, required invasive mechanical ventilation, or had no pain throughout their ED stay were excluded. Primary outcome was the percentage of patients at ED departure achieving adequate pain control of ≤ 50% of triage level. We performed multivariable logistic regression to assess association between demographic and clinical variables with inadequate pain control.
Results: We included 112 patients from 39 different EDs who met inclusion criteria. Mean pain score at triage and ED departure was 8 (standard deviation 8 and 5 [3]), respectively. Median of total morphine equivalent unit (MEU) was 7.5 [5-13] and MEU/kg total body weight (TBW) was 0.09 [0.05-0.16] MEU/kg, with median number of pain medication administration of 2 [1-3] doses. Time interval from triage to first narcotic dose was 61 (35-177) minutes. Overall, only 38% of patients achieved adequate pain control. Among different variables, only total MEU/kg was associated with significant lower risk of inadequate pain control at ED departure (adjusted odds ratio = 0.22; 95% confidence interval = 0.05-0.92, p = 0.037).
Conclusion: Pain control among a group of interhospital-transferred patients requiring urgent operative interventions, was inadequate. Neither demographic nor clinical factors, except MEU/kg TBW, were shown to associate with poor pain management at ED departure. Emergency providers should consider more effective strategies, such as multimodal analgesia, to improve pain management in this group of patients.
Conflict of interest statement
Conflicts of Interest: By the WestJEM article submission agreement, all authors are required to disclose all affiliations, funding sources and financial or management relationships that could be perceived as potential sources of bias. No author has professional or financial relationships with any companies that are relevant to this study. There are no conflicts of interest or sources of funding to declare.
Figures
Similar articles
-
Severe pain management in the emergency department: patient pathway as a new factor associated with IV morphine prescription.Front Public Health. 2024 Feb 22;12:1352833. doi: 10.3389/fpubh.2024.1352833. eCollection 2024. Front Public Health. 2024. PMID: 38454991 Free PMC article.
-
The Critical Care Resuscitation Unit Transfers More Patients From Emergency Departments Faster and Is Associated With Improved Outcomes.J Emerg Med. 2020 Feb;58(2):280-289. doi: 10.1016/j.jemermed.2019.09.041. Epub 2019 Nov 22. J Emerg Med. 2020. PMID: 31761462
-
Factors that affect pain management in adults diagnosed with acute appendicitis in the emergency department: A retrospective study.Am J Emerg Med. 2023 Sep;71:31-36. doi: 10.1016/j.ajem.2023.05.038. Epub 2023 Jun 1. Am J Emerg Med. 2023. PMID: 37327709
-
Triage-initiated intranasal fentanyl for hip fractures in an Emergency Department - Results from introduction of an analgesic guideline.Int Emerg Nurs. 2024 Jun;74:101445. doi: 10.1016/j.ienj.2024.101445. Epub 2024 Apr 4. Int Emerg Nurs. 2024. PMID: 38579496 Review.
-
Canadian nurse initiated analgesia protocol to reduce delays in the emergency department: A quality improvement study.Int Emerg Nurs. 2024 Aug;75:101488. doi: 10.1016/j.ienj.2024.101488. Epub 2024 Jul 12. Int Emerg Nurs. 2024. PMID: 39002430 Review.
Cited by
-
Factors associated with refractory pain in emergency patients admitted to emergency general surgery.World J Emerg Med. 2021;12(1):12-17. doi: 10.5847/wjem.j.1920-8642.2021.01.002. World J Emerg Med. 2021. PMID: 33505544 Free PMC article.
References
-
- Johnston CC, Gagnon AJ, Fullerton L, et al. One-week survey of pain intensity on admission to and discharge from the emergency department: A pilot study. J Emerg Med. 1998;16(3):377–82. - PubMed
-
- Cordell WH, Keene KK, Giles BK, et al. The high prevalence of pain in emergency medical care. Am J Emerg Med. 2002;20(3):165–9. - PubMed
-
- Lanser P, Gesell S. Pain management: the fifth vital sign. Healthc Benchmarks. 2001;8(6):68–70. - PubMed
-
- Todd KH, Ducharme J, Choiniere M, et al. Pain in the emergency department: results of the pain and emergency medicine initiative (PEMI) multicenter study. J Pain. 2007;8(6):460–6. - PubMed
-
- Connor AB, Zwemer FL, Hays DP, et al. Outcomes after intravenous opioids in emergency patients: a prospective cohort analysis. Acad Emerg Med. 2009;16(6):477–87. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous