

The King-Devick test of rapid number naming for concussion detection: meta-analysis and systematic review of the literature
- PMID: 30202552
- PMCID: PMC6114024
- DOI: 10.2217/cnc.15.8
The King-Devick test of rapid number naming for concussion detection: meta-analysis and systematic review of the literature
Abstract
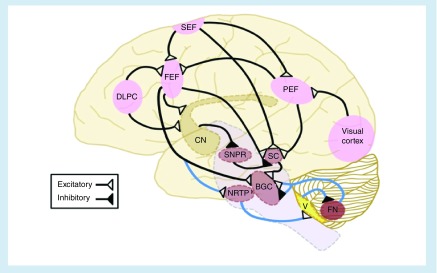
Background: Vision encompasses a large component of the brain's pathways, yet is not represented in current sideline testing.
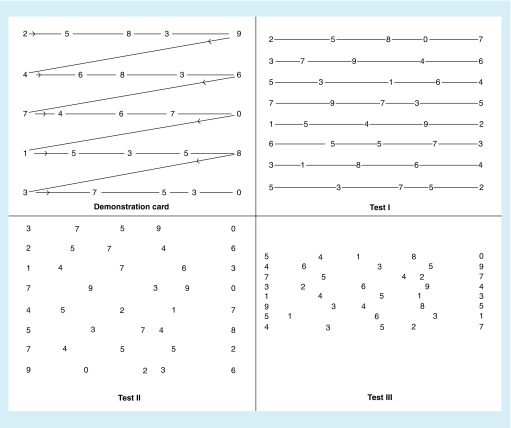
Objectives: We performed a meta-analysis of published data for a vision-based test of rapid number naming (King-Devick [K-D] test).
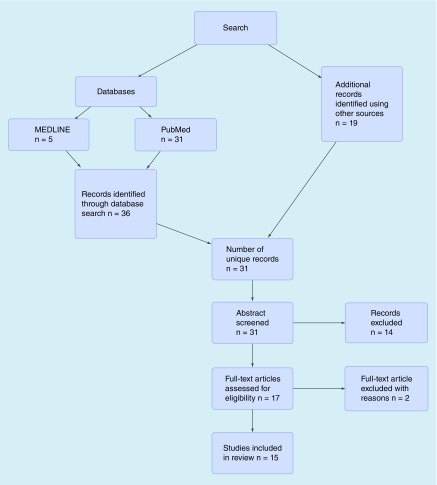
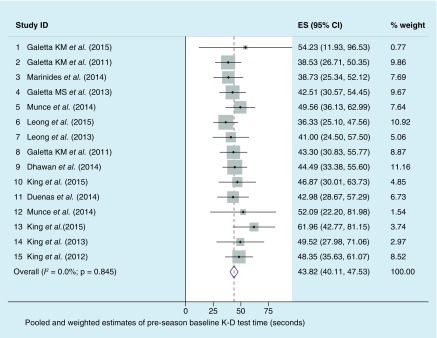
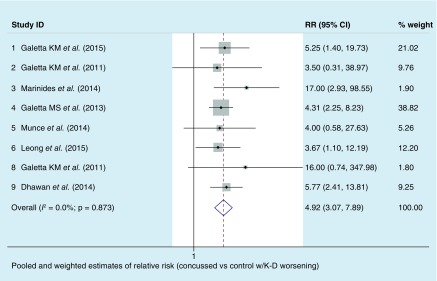
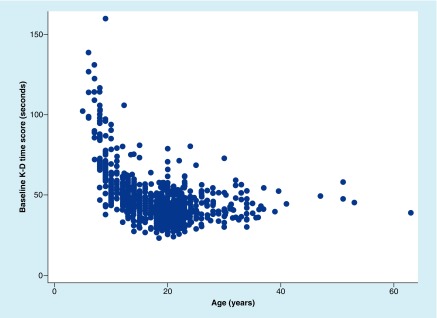
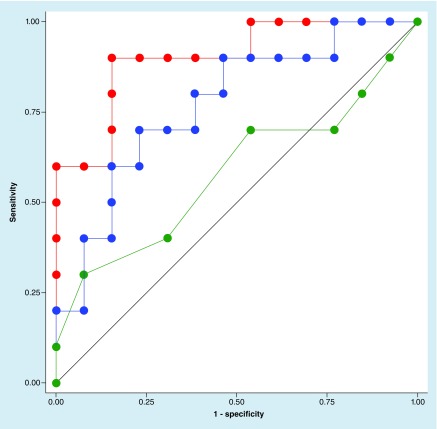
Studies & methods: Pooled and meta-analysis of 15 studies estimated preseason baseline K-D scores and sensitivity/specificity for identifying concussed versus nonconcussed control athletes.
Result: Baseline K-D (n = 1419) showed a weighted estimate of 43.8 s (95% CI: 40.2, 47.5; I2 = 0.0%; p=0.85 - indicating very little heterogeneity). Sensitivity was 86% (96/112 concussed athletes had K-D worsening; 95% CI: 78%, 92%); specificity was 90% (181/202 controls had no worsening; 95% CI: 85%, 93%).
Conclusion: Rapid number naming adds to sideline assessment and contributes a critical dimension of vision to sports-related concussion testing.
Keywords: King-Devick test; concussion; meta-analysis; rapid number naming; saccades; sports; vision.
Conflict of interest statement
Financial & competing interests disclosure S Galetta has received consulting honoraria from Biogen and Genzyme. LJ Balcer has received consulting honoraria from Biogen and Genzyme, and has served on a clinical trial advisory board for Biogen. DF Leong is an employee of King-Devick Test, Inc. The authors have no other relevant affiliations or financial involvement with any organization or entity with a financial interest in or financial conflict with the subject matter or materials discussed in the manuscript apart from those disclosed. No writing assistance was utilized in the production of this manuscript.
Figures
References
-
- McCrory P, Meeuwisse WH, Aubry M, et al. Consensus statement on concussion in sport: the 4th International Conference on Concussion in Sport held in Zurich, November 2012. Br. J. Sports Med. 2013;47(5):250–258. - PubMed
-
- Plassman BL, Havlik RJ, Steffens DC, et al. Documented head injury in early adulthood and risk of Alzheimer's disease and other dementias. Neurology. 2000;55(8):1158–1166. - PubMed
-
- Eibner C, Schell TL, Jaycox LH. Care of war veterans with mild traumatic brain injury. N. Engl. J. Med. 2009;361(5):537. author reply 537–538. - PubMed
-
- Xydakis MS, Robbins AS, Grant GA. Mild traumatic brain injury in U.S. soldiers returning from Iraq. N. Engl. J. Med. 2008;358(20):2177. author reply 2179. - PubMed
-
- Walsh DV, Capó-Aponte JE, Jorgensen-Wagers K, et al. Visual field dysfunctions in warfighters during different stages following blast and nonblast mTBI. Mil. Med. 2015;180(2):178–185. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical