

Investigation of postoperative hypernasality after superiorly based posterior pharyngeal flap
- PMID: 30202766
- PMCID: PMC6115315
- DOI: 10.1186/s40902-018-0164-2
Investigation of postoperative hypernasality after superiorly based posterior pharyngeal flap
Abstract
Background: Velopharyngeal insufficiency that accompanies speech resonance and articulation disorders can be managed through several intervention methods such as speech-language therapy, prosthetic aids, and surgery. However, for patients with severe hypernasality, surgical interventions are highly recommended. Among available surgical techniques, the posterior pharyngeal flap is most common.
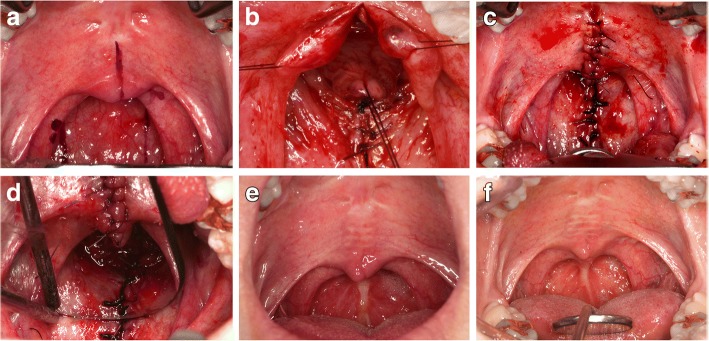
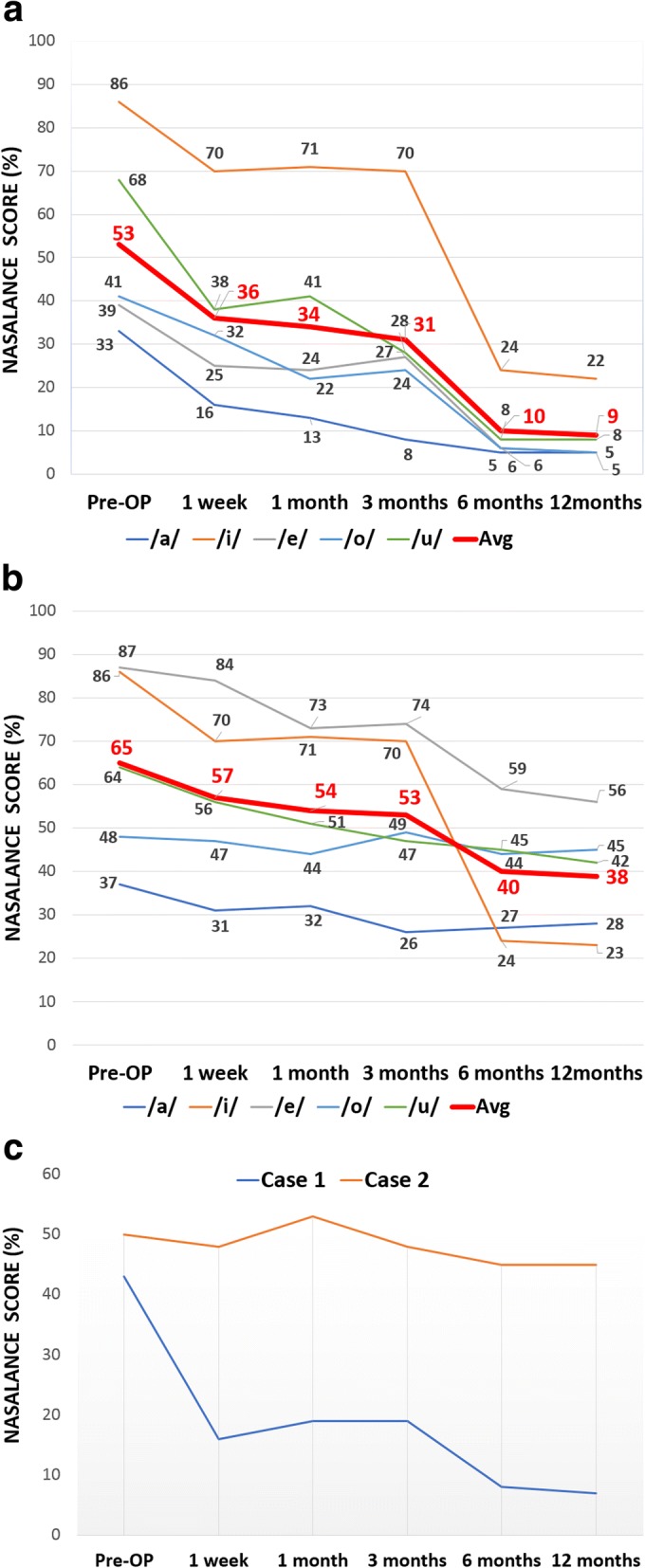
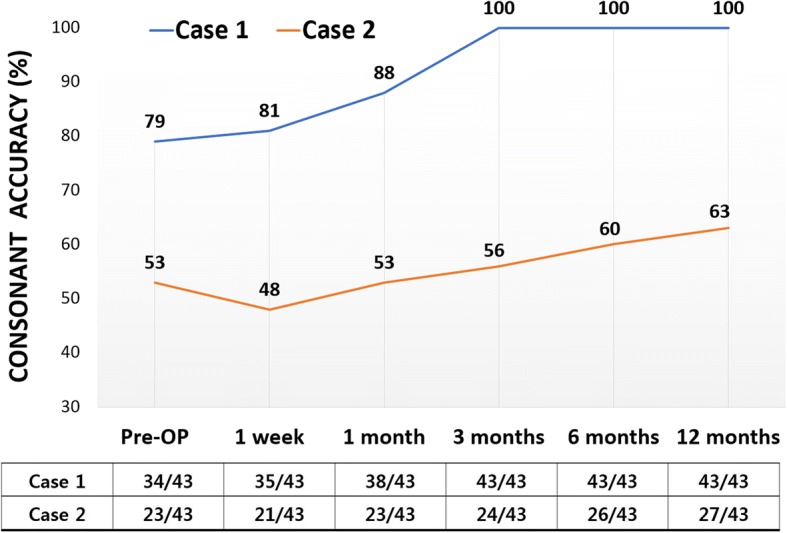
Case presentation: Two adult males with high nasalance scores underwent superiorly based posterior pharyngeal flap surgery, followed by speech testing by an expert speech-language therapist. Nasalance scores and articulation accuracy were assessed up until 1 year after the surgery. Nasalance scores were measured five times using a nasometer, after which the average value was calculated.
Conclusions: Consistent declines in hypernasality over time are not easy to explain since the pedicled pharyngeal flap narrowed over time, secondary to cicatrization. However, scar tethering of the soft palate in a posterior direction could reduce the velopharyngeal port size over time. Therefore, long-term follow-up with intensive speech therapy is suggested for patients with severe hypernasality.
Keywords: Cleft palate; Nasalance; Nasometer; Pharyngoplasty; Posterior pharyngeal flap.
Conflict of interest statement
The practice and the report of cases have been performed in accordance with the Declaration of Helsinki. Ethics approval of report involving less than three cases is waved.Written informed consent was obtained from the patient for publication of this case report and accompanying images.The authors declare that they have no competing interests. All of the authors have no affiliations with or involvement in any organization or entity with any financial interest or non-financial interest in this manuscript.Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures

References
-
- Peterson-Falzone SJ, Hardin-Jones MA, Karnell MP. The clinician’s guide to treating cleft palate speech. St. Louis: Mosby; 2006.
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources