

Cardiotoxicity with vascular endothelial growth factor inhibitor therapy
- PMID: 30202791
- PMCID: PMC5988734
- DOI: 10.1038/s41698-018-0056-z
Cardiotoxicity with vascular endothelial growth factor inhibitor therapy
Abstract
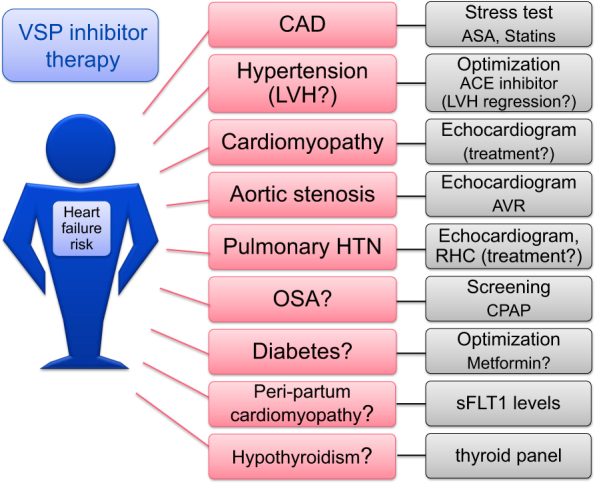
Angiogenesis inhibitors targeting the vascular endothelial growth factor (VEGF) signaling pathway (VSP) have been important additions in the therapy of various cancers, especially renal cell carcinoma and colorectal cancer. Bevazicumab, the first VSP to receive FDA approval in 2004 targeting all circulating isoforms of VEGF-A, has become one of the best-selling drugs of all times. The second wave of tyrosine kinase inhibitors (TKIs), which target the intracellular site of VEGF receptor kinases, began with the approval of sorafenib in 2005 and sunitinib in 2006. Heart failure was subsequently noted, in 2-4% of patients on bevacizumab and in 3-8% of patients on VSP-TKIs. The very fact that the single-targeted monoclonal antibody bevacizumab can induce cardiotoxicity supports a pathomechanistic role for the VSP and the postulate of the "vascular" nature of VSP inhibitor cardiotoxicity. In this review we will outline this scenario in greater detail, reflecting on hypertension and coronary artery disease as risk factors for VSP inhibitor cardiotoxicity, but also similarities with peripartum and diabetic cardiomyopathy. This leads to the concept that any preexisting or coexisting condition that reduces the vascular reserve or utilizes the vascular reserve for compensatory purposes may pose a risk factor for cardiotoxicity with VSP inhibitors. These conditions need to be carefully considered in cancer patients who are to undergo VSP inhibitor therapy. Such vigilance is not to exclude patients from such prognostically extremely important therapy but to understand the continuum and to recognize and react to any cardiotoxicity dynamics early on for superior overall outcomes.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Seto T, et al. Erlotinib alone or with bevacizumab as first-line therapy in patients with advanced non-squamous non-small-cell lung cancer harbouring EGFR mutations (JO25567): an open-label, randomised, multicentre, phase 2 study. Lancet Oncol. 2014;15:1236–1244. doi: 10.1016/S1470-2045(14)70381-X. - DOI - PubMed
-
- Conti E, et al. Arterial thrombotic events and acute coronary syndromes with cancer drugs: are growth factors the missed link?: what both cardiologist and oncologist should know about novel angiogenesis inhibitors. Int J. Cardiol. 2013;167:2421–2429. doi: 10.1016/j.ijcard.2013.01.052. - DOI - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
