

Initial toxicity, quality-of-life outcomes, and dosimetric impact in a randomized phase 3 trial of hypofractionated versus standard fractionated proton therapy for low-risk prostate cancer
- PMID: 30202801
- PMCID: PMC6128091
- DOI: 10.1016/j.adro.2018.02.004
Initial toxicity, quality-of-life outcomes, and dosimetric impact in a randomized phase 3 trial of hypofractionated versus standard fractionated proton therapy for low-risk prostate cancer
Abstract
Purpose: Randomized evidence for extreme hypofractionation in prostate cancer is lacking. We aimed to identify differences in toxicity and quality-of-life outcomes between standard fractionation and extreme hypofractionated radiation in a phase 3 randomized trial.
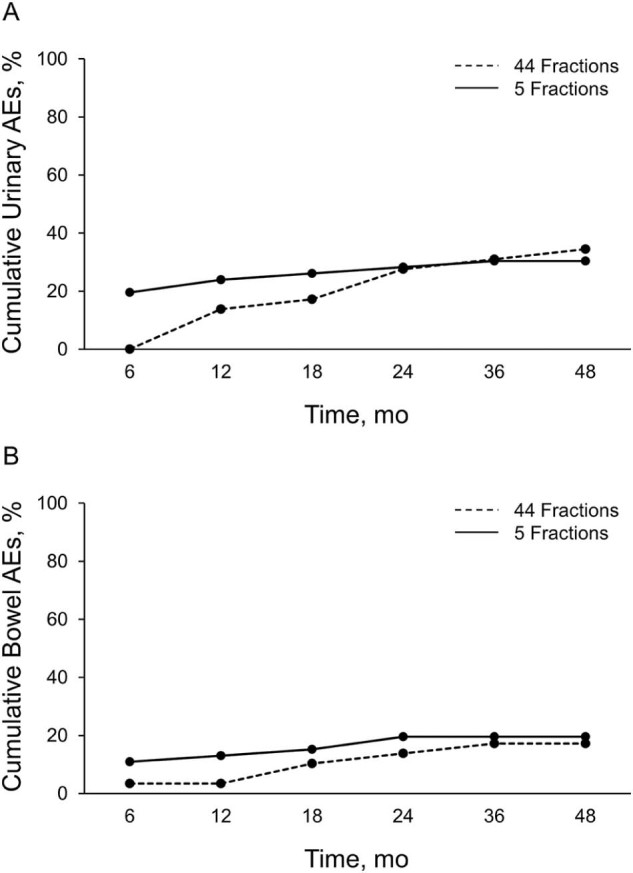
Methods and materials: We analyzed the results of the first 75 patients in our phase 3 trial, comparing 38 Gy relative biologic effectiveness (RBE) in 5 fractions (n = 46) versus 79.2 Gy RBE in 44 fractions (n = 29). Patients received proton radiation using fiducials and daily image guidance. We evaluated American Urological Association Symptom Index (AUASI), adverse events (AEs), and Expanded Prostate Index Composite (EPIC) domains. The primary endpoint of this interim analysis was the cumulative incidence of grade 2 (G2) or higher AEs. The randomized patient allocation scheme was a 2:1 ratio favoring the 38 Gy RBE arm.
Results: The median follow-up was 36 months; 30% of patients reached 48-month follow-up. AUASI scores differed <5 points (4.4 vs 8.6; P = .002) at 1 year, favoring the 79.2 Gy arm. Differences in AUASI were not significant at ≥18 months. EPIC urinary symptoms favored the 79.2 Gy arm at 1 year (92.3 vs 84.5; P = .009) and 18 months (92.3 vs 85.3; P = .03); bother scores were not significant at other time points. Cumulative ≥G2 genitourinary toxicity was similar between the 79.2 Gy and 38 Gy arms (34.5% vs 30.4%; P = .80). We found no differences in the EPIC domains of bowel symptoms, sexual symptoms, or bowel ≥G2 toxicities. Bladder V80 (79.2 Gy arm; P = .04) and V39 (38 Gy arm; P = .05) were predictive for cumulative G2 genitourinary AEs.
Conclusions: Low AE rates were seen in both study arms. Early temporary differences in genitourinary scores disappeared over time. Bladder constraints were associated with genitourinary AEs.
Figures
Similar articles
-
Hypofractionated Versus Standard Fractionated Proton-beam Therapy for Low-risk Prostate Cancer: Interim Results of a Randomized Trial PCG GU 002.Am J Clin Oncol. 2018 Feb;41(2):115-120. doi: 10.1097/COC.0000000000000241. Am J Clin Oncol. 2018. PMID: 26523442 Clinical Trial.
-
Image-guided hypofractionated proton beam therapy for low-risk prostate cancer: Analysis of quality of life and toxicity, PCG GU 002.Rep Pract Oncol Radiother. 2016 May-Jun;21(3):207-12. doi: 10.1016/j.rpor.2016.01.002. Epub 2016 Mar 4. Rep Pract Oncol Radiother. 2016. PMID: 27601952 Free PMC article.
-
Hypofractionated versus conventionally fractionated radiotherapy for patients with prostate cancer (HYPRO): acute toxicity results from a randomised non-inferiority phase 3 trial.Lancet Oncol. 2015 Mar;16(3):274-83. doi: 10.1016/S1470-2045(14)70482-6. Epub 2015 Feb 3. Lancet Oncol. 2015. PMID: 25656287 Clinical Trial.
-
A randomized hypofractionation dose escalation trial for high risk prostate cancer patients: interim analysis of acute toxicity and quality of life in 124 patients.Radiat Oncol. 2013 Sep 4;8:206. doi: 10.1186/1748-717X-8-206. Radiat Oncol. 2013. PMID: 24007322 Free PMC article. Clinical Trial.
-
Hypofractionation for clinically localized prostate cancer.Cochrane Database Syst Rev. 2019 Sep 3;9(9):CD011462. doi: 10.1002/14651858.CD011462.pub2. Cochrane Database Syst Rev. 2019. PMID: 31476800 Free PMC article.
Cited by
-
Dosimetric feasibility of moderately hypofractionated/dose escalated radiation therapy for localised prostate cancer with intensity-modulated proton beam therapy using simultaneous integrated boost (SIB-IMPT) and impact of hydrogel prostate-rectum spacer.Radiat Oncol. 2022 Apr 1;17(1):64. doi: 10.1186/s13014-022-02025-2. Radiat Oncol. 2022. PMID: 35365170 Free PMC article.
-
The Status and Challenges for Prostate Stereotactic Body Radiation Therapy Treatments in United States Proton Therapy Centers: An NRG Oncology Practice Survey.Int J Part Ther. 2024 Apr 24;11:100020. doi: 10.1016/j.ijpt.2024.100020. eCollection 2024 Mar. Int J Part Ther. 2024. PMID: 38757080 Free PMC article.
-
The Case for Brachytherapy: Why It Deserves a Renaissance.Adv Radiat Oncol. 2021 Mar-Apr;6(2):100605. doi: 10.1016/j.adro.2020.10.018. Epub 2020 Nov 6. Adv Radiat Oncol. 2021. PMID: 33723523 Free PMC article.
-
Radiotherapy-related toxicity for localized prostate cancer: meta-analysis comparing conventional or moderately hypofractionated vs. ultrahypofractionated protocols.Clin Transl Oncol. 2022 Jul;24(7):1425-1439. doi: 10.1007/s12094-022-02790-2. Epub 2022 Mar 4. Clin Transl Oncol. 2022. PMID: 35244866 Review.
-
The Role of Hypofractionation in Proton Therapy.Cancers (Basel). 2022 May 2;14(9):2271. doi: 10.3390/cancers14092271. Cancers (Basel). 2022. PMID: 35565400 Free PMC article. Review.
References
-
- Dearnaley D.P., Jovic G., Syndikus I. Escalated-dose versus control-dose conformal radiotherapy for prostate cancer: Long-term results from the MRC RT01 randomised controlled trial. Lancet Oncol. 2014;15:464–473. - PubMed
-
- Kuban D.A., Levy L.B., Cheung M.R. Long-term failure patterns and survival in a randomized dose-escalation trial for prostate cancer. Who dies of disease? Int J Radiat Oncol Biol Phys. 2011;79:1310–1317. - PubMed
-
- Peeters S.T., Heemsbergen W.D., Koper P.C. Dose-response in radiotherapy for localized prostate cancer: Results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol. 2006;24:1990–1996. - PubMed
-
- Zietman A.L., Bae K., Slater J.D. Randomized trial comparing conventional-dose with high-dose conformal radiation therapy in early-stage adenocarcinoma of the prostate: Long-term results from Proton Radiation Oncology group/American College of Radiology 95-09. J Clin Oncol. 2010;28:1106–1111. - PMC - PubMed
-
- Brenner D.J., Hall E.J. Fractionation and protraction for radiotherapy of prostate carcinoma. Int J Radiat Oncol Biol Phys. 1999;43:1095–1101. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
