

Initial toxicity, quality-of-life outcomes, and dosimetric impact in a randomized phase 3 trial of hypofractionated versus standard fractionated proton therapy for low-risk prostate cancer
- PMID: 30202801
- PMCID: PMC6128091
- DOI: 10.1016/j.adro.2018.02.004
Initial toxicity, quality-of-life outcomes, and dosimetric impact in a randomized phase 3 trial of hypofractionated versus standard fractionated proton therapy for low-risk prostate cancer
Abstract
Purpose: Randomized evidence for extreme hypofractionation in prostate cancer is lacking. We aimed to identify differences in toxicity and quality-of-life outcomes between standard fractionation and extreme hypofractionated radiation in a phase 3 randomized trial.
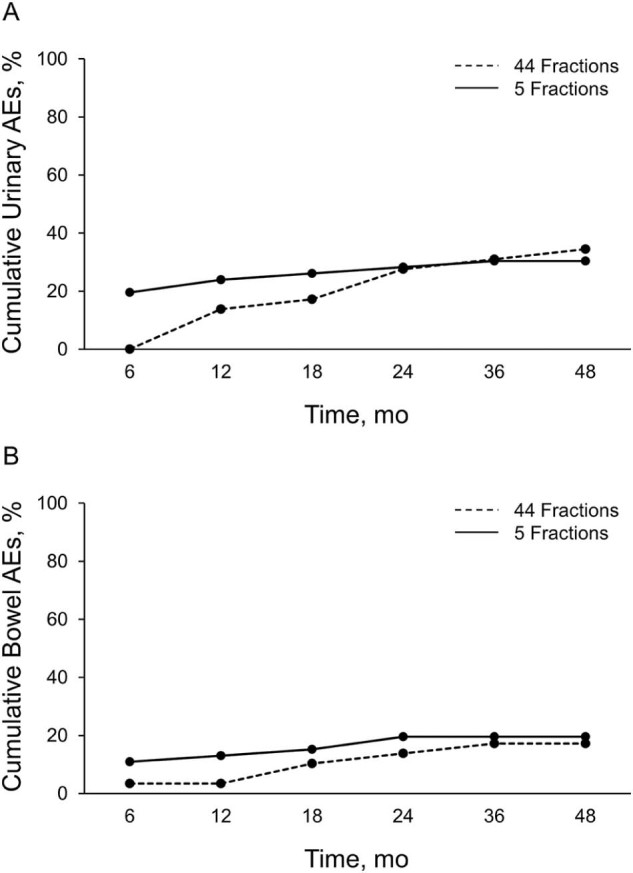
Methods and materials: We analyzed the results of the first 75 patients in our phase 3 trial, comparing 38 Gy relative biologic effectiveness (RBE) in 5 fractions (n = 46) versus 79.2 Gy RBE in 44 fractions (n = 29). Patients received proton radiation using fiducials and daily image guidance. We evaluated American Urological Association Symptom Index (AUASI), adverse events (AEs), and Expanded Prostate Index Composite (EPIC) domains. The primary endpoint of this interim analysis was the cumulative incidence of grade 2 (G2) or higher AEs. The randomized patient allocation scheme was a 2:1 ratio favoring the 38 Gy RBE arm.
Results: The median follow-up was 36 months; 30% of patients reached 48-month follow-up. AUASI scores differed <5 points (4.4 vs 8.6; P = .002) at 1 year, favoring the 79.2 Gy arm. Differences in AUASI were not significant at ≥18 months. EPIC urinary symptoms favored the 79.2 Gy arm at 1 year (92.3 vs 84.5; P = .009) and 18 months (92.3 vs 85.3; P = .03); bother scores were not significant at other time points. Cumulative ≥G2 genitourinary toxicity was similar between the 79.2 Gy and 38 Gy arms (34.5% vs 30.4%; P = .80). We found no differences in the EPIC domains of bowel symptoms, sexual symptoms, or bowel ≥G2 toxicities. Bladder V80 (79.2 Gy arm; P = .04) and V39 (38 Gy arm; P = .05) were predictive for cumulative G2 genitourinary AEs.
Conclusions: Low AE rates were seen in both study arms. Early temporary differences in genitourinary scores disappeared over time. Bladder constraints were associated with genitourinary AEs.
Figures
References
-
- Dearnaley D.P., Jovic G., Syndikus I. Escalated-dose versus control-dose conformal radiotherapy for prostate cancer: Long-term results from the MRC RT01 randomised controlled trial. Lancet Oncol. 2014;15:464–473. - PubMed
-
- Kuban D.A., Levy L.B., Cheung M.R. Long-term failure patterns and survival in a randomized dose-escalation trial for prostate cancer. Who dies of disease? Int J Radiat Oncol Biol Phys. 2011;79:1310–1317. - PubMed
-
- Peeters S.T., Heemsbergen W.D., Koper P.C. Dose-response in radiotherapy for localized prostate cancer: Results of the Dutch multicenter randomized phase III trial comparing 68 Gy of radiotherapy with 78 Gy. J Clin Oncol. 2006;24:1990–1996. - PubMed
-
- Zietman A.L., Bae K., Slater J.D. Randomized trial comparing conventional-dose with high-dose conformal radiation therapy in early-stage adenocarcinoma of the prostate: Long-term results from Proton Radiation Oncology group/American College of Radiology 95-09. J Clin Oncol. 2010;28:1106–1111. - PMC - PubMed
-
- Brenner D.J., Hall E.J. Fractionation and protraction for radiotherapy of prostate carcinoma. Int J Radiat Oncol Biol Phys. 1999;43:1095–1101. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
