

Late toxicity after post-prostatectomy intensity modulated radiation therapy: Evaluating normal-tissue sparing guidelines
- PMID: 30202803
- PMCID: PMC6128032
- DOI: 10.1016/j.adro.2018.04.009
Late toxicity after post-prostatectomy intensity modulated radiation therapy: Evaluating normal-tissue sparing guidelines
Abstract
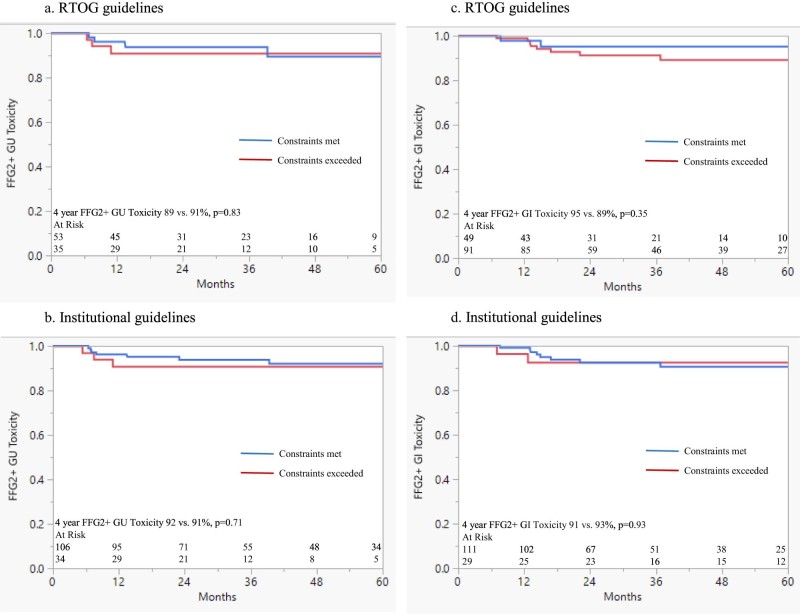
Purpose: Dose-volume histogram (DVH) toxicity relationships are poorly defined in men who receive radiation after radical prostatectomy (RP). We evaluated Radiation Therapy Oncology Group (RTOG) study 0534 and institutional intact normal-tissue sparing guidelines, as well as dose to bladder trigone, for ability to minimize late toxicity.
Methods and materials: 164 men received intensity modulated radiation therapy (RT) to a median prostate bed dose of 66.6 Gy at a median of 22 months after RP. 46% of men were prescribed androgen deprivation therapy and pelvic lymph node irradiation to a median dose of 50.4 Gy. DVH relationships for the rectum, bladder, trigone, and bladder excluding the clinical target volume (bladder-CTV) were analyzed against the Common Terminology Criteria for Adverse Events late grade 2 + (G2+) gastrointestinal (GI) and genitourinary (GU) toxicity by log-rank test. RTOG 0534 (rectum V65, 40 Gy ≤35, 55%, and bladder-CTV V65, 40 ≤50, 70%) and intact prostate RT institutional guidelines (rectum V70, 65, 40 ≤20, 40, 80% and bladder V70, 65, 40 ≤30, 60, 80%, respectively) guidelines were evaluated.
Results: With a median follow-up time of of 33 months, the 4-year freedom from G2 + GI and GU toxicity were both 91%. G2 + GI (n = 12) and GU (n = 15) toxicity included 4% diarrhea (n = 6), 4% hemorrhage (n = 6), 1% proctitis (n = 1), and 4% urinary frequency (n = 7), 1% obstructive (n = 2), 2% cystitis (n = 3), and 3% incontinence (n = 5), respectively. RTOG 0534 rectum and bladder goals were not achieved in 65% and 41% of cases, while the institutional intact prostate goals were not achieved in 21% and 25% of cases, respectively. Neither dose to the bladder trigone nor any of the proposed normal tissue goals were associated with late toxicity (P > .1). In the univariate analysis, age, pelvic RT, RT dose, anticoagulation use, androgen deprivation therapy, time from RP to RT, and tobacco history were not associated with toxicity.
Conclusions: More than 90% of men were free from late G2 + toxicity 4 years after post-RP intensity modulated RT. No tested parameters were associated with late toxicity. In the absence of established normal-tissue DVH guidelines in the postoperative setting, the use of intact guidelines is reasonable.
Figures
References
-
- Bolla M., van Poppel H., Tombal B. Postoperative radiotherapy after radical prostatectomy for high-risk prostate cancer: Long-term results of a randomised controlled trial (EORTC trial 22911) Lancet. 2012;380:2018–2027. - PubMed
-
- Wiegel T., Bartkowiak D., Bottke D. Adjuvant radiotherapy versus wait-and-see after radical prostatectomy: 10-year follow-up of the ARO 96-02/AUO AP 09/95 trial. Eur Urol. 2014;66:243–250. - PubMed
-
- Shipley W., Seiferheld W., Lukka H. Report of NRG Oncology/RTOG 9601, A phase 3 trial in prostate cancer: Anti-androgen therapy (AAT) with bicalutamide during and after radiation therapy (RT) in patients following radical prostatectomy (RP) with pT2-3pN0 disease and an elevated PSA. Int J Radiat Oncol Biol Phys. 2016;94:3–6.
LinkOut - more resources
Full Text Sources
Other Literature Sources
