

Definitive hypofractionated radiation therapy for early stage breast cancer: Dosimetric feasibility of stereotactic ablative radiotherapy and proton beam therapy for intact breast tumors
- PMID: 30202812
- PMCID: PMC6128030
- DOI: 10.1016/j.adro.2018.05.002
Definitive hypofractionated radiation therapy for early stage breast cancer: Dosimetric feasibility of stereotactic ablative radiotherapy and proton beam therapy for intact breast tumors
Abstract
Purpose: Few definitive treatment options exist for elderly patients diagnosed with early stage breast cancer who are medically inoperable or refuse surgery. Historical data suggest very poor local control with hormone therapy alone. We examined the dosimetric feasibility of hypofractionated radiation therapy using stereotactic ablative radiotherapy (SABR) and proton beam therapy (PBT) as a means of definitive treatment for early stage breast cancer.
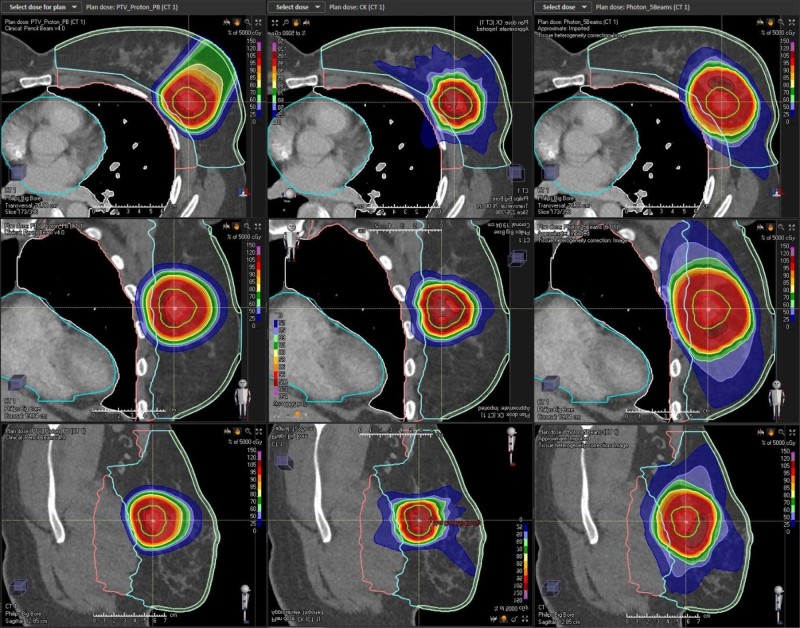
Methods and materials: Fifteen patients with biopsy-proven early stage breast cancer with a clinically visible tumor on preoperative computed tomography scans were identified. Gross tumor volumes were contoured and correlated with known biopsy-proven malignancy on prior imaging. Treatment margins were created on the basis of set-up uncertainty and image guidance capabilities of the three radiation modalities analyzed (3-dimensional conformal radiation therapy [3D-CRT], SABR, and PBT) to deliver a total dose of 50 Gy in 5 fractions. Dose volume histograms were analyzed and compared between treatment techniques.
Results: The median planning target volume (PTV) for SABR, PBT, and 3-dimensional CRT was 11.91, 21.03, and 45.08 cm3, respectively, and were significantly different (P < .0001) between treatment modalities. Overall target coverage of gross tumor and clinical target volumes was excellent with all three modalities. Both SABR and PBT demonstrated significant dosimetric improvements, each in its own unique manner, relative to 3D-CRT. Dose constraints to normal structures including ipsilateral/contralateral breast, bilateral lungs, and heart were all consistently achieved using SABR and PBT. However, skin or chest wall dose constraints were exceeded in some cases for both SABR and PBT plans and was dictated by the anatomic location of the tumor.
Conclusions: Definitive hypofractionated radiation therapy using SABR and PBT appears to be dosimetrically feasible for the treatment of early stage breast cancer. The anatomical location of the tumor relative to the skin and chest wall appears to be the primary limiting dosimetric factor.
Figures



 ), proton beam therapy (+), and stereotactic ablative radiation surgery (x).
), proton beam therapy (+), and stereotactic ablative radiation surgery (x).Similar articles
-
A treatment planning comparison of photon stereotactic ablative radiotherapy and proton beam therapy for the re-irradiation of pelvic cancer recurrence.Phys Imaging Radiat Oncol. 2022 Feb 23;21:78-83. doi: 10.1016/j.phro.2022.02.010. eCollection 2022 Jan. Phys Imaging Radiat Oncol. 2022. PMID: 35243036 Free PMC article.
-
Accelerated partial breast irradiation: a dosimetric comparison of three different techniques.Brachytherapy. 2005;4(2):121-9. doi: 10.1016/j.brachy.2004.12.005. Brachytherapy. 2005. PMID: 15893265
-
Dosimetric Comparisons between Proton Beam Therapy and Modern Photon Radiation Techniques for Stage I Non-Small Cell Lung Cancer According to Tumor Location.Cancers (Basel). 2021 Dec 17;13(24):6356. doi: 10.3390/cancers13246356. Cancers (Basel). 2021. PMID: 34944976 Free PMC article.
-
Proton therapy for early-stage non-small cell lung cancer (NSCLC).Transl Lung Cancer Res. 2018 Apr;7(2):199-204. doi: 10.21037/tlcr.2018.04.12. Transl Lung Cancer Res. 2018. PMID: 29876319 Free PMC article. Review.
-
Accelerated dose escalation with proton beam therapy for non-small cell lung cancer.J Thorac Dis. 2014 Apr;6(4):348-55. doi: 10.3978/j.issn.2072-1439.2013.11.07. J Thorac Dis. 2014. PMID: 24688779 Free PMC article. Review.
Cited by
-
Treatment Options for Early Stage Inoperable Breast Cancer: Cryoablation or Radiotherapy?Breast Care (Basel). 2024 Apr;19(2):106-115. doi: 10.1159/000536413. Epub 2024 Jan 22. Breast Care (Basel). 2024. PMID: 38645759 Free PMC article. Review.
-
The role of proton beam therapy in the management of elderly breast cancer patients.Transl Cancer Res. 2020 Jan;9(Suppl 1):S161-S172. doi: 10.21037/tcr.2019.07.40. Transl Cancer Res. 2020. PMID: 35117960 Free PMC article. Review.
-
A narrative review for radiation oncologists to implement preoperative partial breast irradiation.Radiol Med. 2023 Dec;128(12):1553-1570. doi: 10.1007/s11547-023-01706-6. Epub 2023 Aug 31. Radiol Med. 2023. PMID: 37650981 Review.
-
Breast radiotherapy in elderly women: myths, controversies, and current techniques in the adjuvant setting.Transl Cancer Res. 2020 Jan;9(Suppl 1):S37-S55. doi: 10.21037/tcr.2019.07.09. Transl Cancer Res. 2020. PMID: 35117947 Free PMC article. Review.
-
Hypofractionated proton therapy in breast cancer: where are we? A critical review of the literature.Breast Cancer Res Treat. 2022 Apr;192(2):249-263. doi: 10.1007/s10549-022-06516-4. Epub 2022 Jan 13. Breast Cancer Res Treat. 2022. PMID: 35025004 Review.
References
-
- Crivellari D., Aapro M., Leonard R. Breast cancer in the elderly. J Clin Oncol. 2007;25:1882–1890. - PubMed
-
- de Glas N.A., Jonker J.M., Bastiaannet E. Impact of omission of surgery on survival of older patients with breast cancer. Br J Surg. 2014;101:1397–1404. - PubMed
-
- Hughes K.S., Schnaper L.A., Berry D. Lumpectomy plus tamoxifen with or without irradiation in women 70 years of age or older with early breast cancer. N Engl J Med. 2004;351:971–977. - PubMed
-
- Fyles A.W., McCready D.R., Manchul L.A. Tamoxifen with or without breast irradiation in women 50 years of age or older with early breast cancer. N Engl J Med. 2004;351:963–970. - PubMed
-
- Louwman W.J., Janssen-Heijnen M.L., Houterman S. Less extensive treatment and inferior prognosis for breast cancer patient with comorbidity: A population-based study. Eur J Cancer. 2005;41:779–785. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
