

An Increase in Chromogranin A-Positive, Hormone-Negative Endocrine Cells in Pancreas in Cystic Fibrosis
- PMID: 30202828
- PMCID: PMC6125715
- DOI: 10.1210/js.2018-00143
An Increase in Chromogranin A-Positive, Hormone-Negative Endocrine Cells in Pancreas in Cystic Fibrosis
Abstract
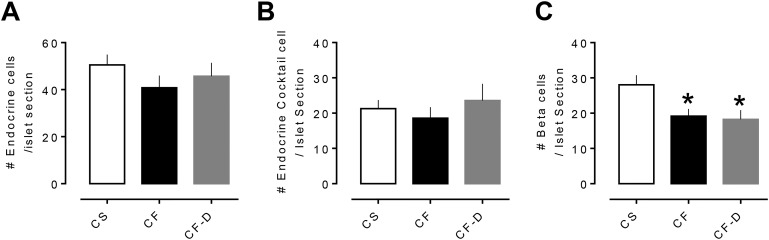
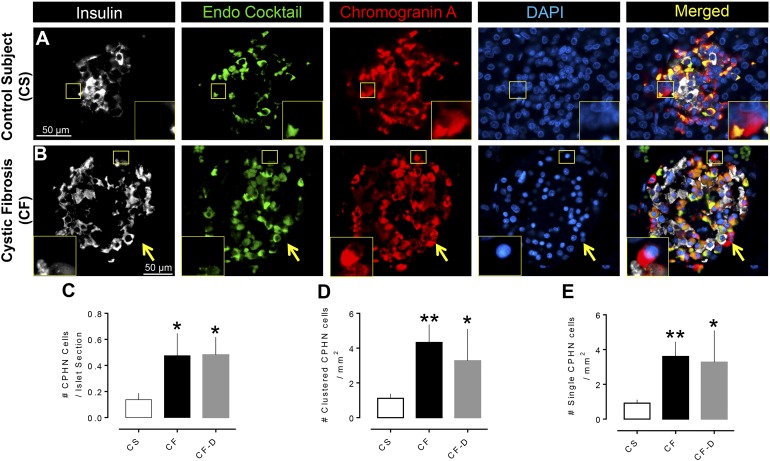
We sought to establish whether an increase in chromogranin A-positive, hormone-negative (CPHN) endocrine cells occurs in the pancreas of patients with cystic fibrosis (CF), as potential evidence of neogenesis. Pancreata were obtained at autopsy from nondiabetic patients with CF (n = 12) and age-matched nondiabetic control subject (CS) individuals without CF (n = 12). In addition, pancreas from three diabetic patients with CF was obtained. Pancreas sections were stained for chromogranin A, insulin, and a cocktail of glucagon, somatostatin, pancreatic polypeptide, and ghrelin and evaluated for the frequency of CPHN cells. There was a higher frequency of CPHN cells in islets of the patients with CF compared with the CS group. Moreover, CPHN cells occurring as single cells or clusters scattered in the exocrine pancreas were also more frequent in patients with CF. The increased frequency of CPHN cells in pancreas of patients with CF may indicate an attempt at endocrine cell regeneration.
Keywords: cystic fibrosis; inflammation; β cell.
Figures
References
-
- O’Sullivan BP, Freedman SD. Cystic fibrosis. Lancet. 2009;373(9678):1891–1904. - PubMed
-
- Riordan JR, Rommens JM, Kerem B, Alon N, Rozmahel R, Grzelczak Z, Zielenski J, Lok S, Plavsic N, Chou JL, Drumm ML, Iannuzzi MC, Collins FS, Tsui L-C. Identification of the cystic fibrosis gene: cloning and characterization of complementary DNA. Science. 1989;245(4922):1066–1073. - PubMed
-
- Hasegawa H, Skach W, Baker O, Calayag MC, Lingappa V, Verkman AS. A multifunctional aqueous channel formed by CFTR. Science. 1992;258(5087):1477–1479. - PubMed
-
- di Sant’Agnese PA, Davis PB. Cystic fibrosis in adults: 75 cases and a review of 232 cases in the literature. Am J Med. 1979;66(1):121–132. - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials