

Guideline-indicated treatments and diagnostics, GRACE risk score, and survival for non-ST elevation myocardial infarction
- PMID: 30202849
- PMCID: PMC6220125
- DOI: 10.1093/eurheartj/ehy517
Guideline-indicated treatments and diagnostics, GRACE risk score, and survival for non-ST elevation myocardial infarction
Abstract
Aims: To investigate whether improved survival from non-ST-elevation myocardial infarction (NSTEMI), according to GRACE risk score, was associated with guideline-indicated treatments and diagnostics, and persisted after hospital discharge.
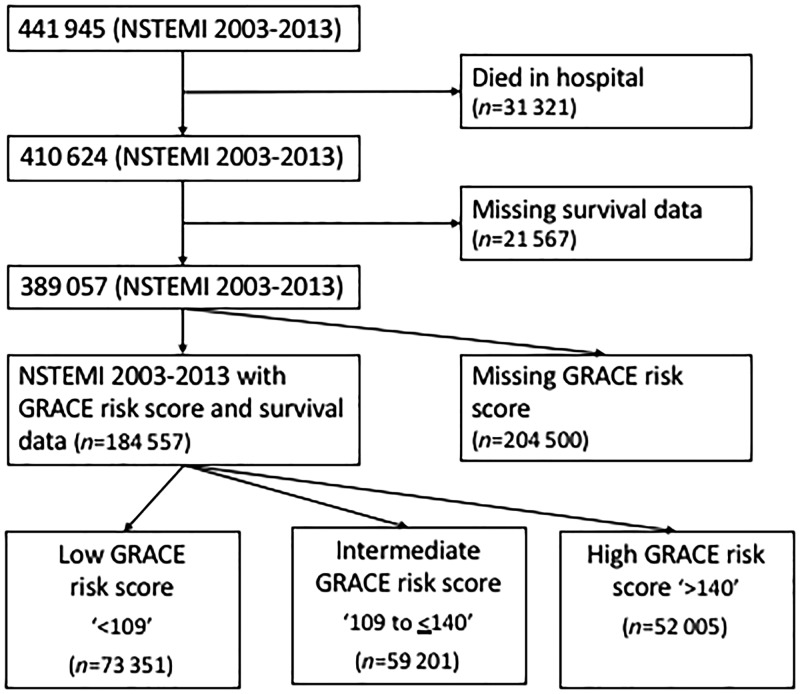
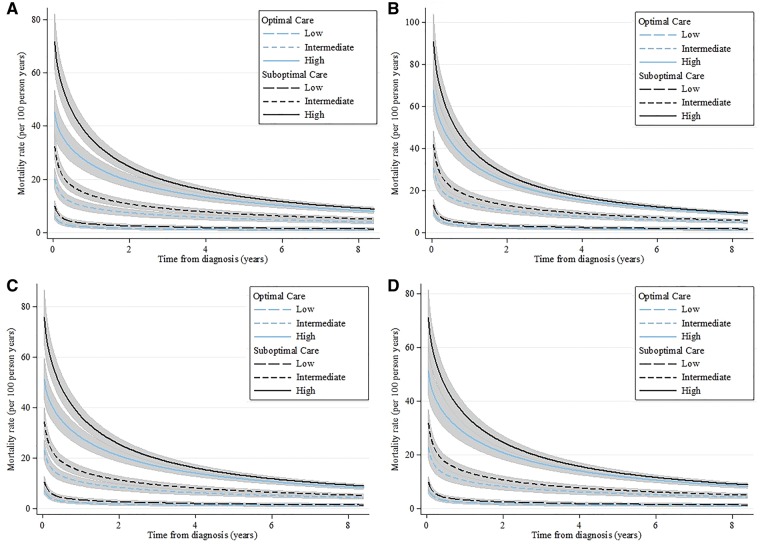
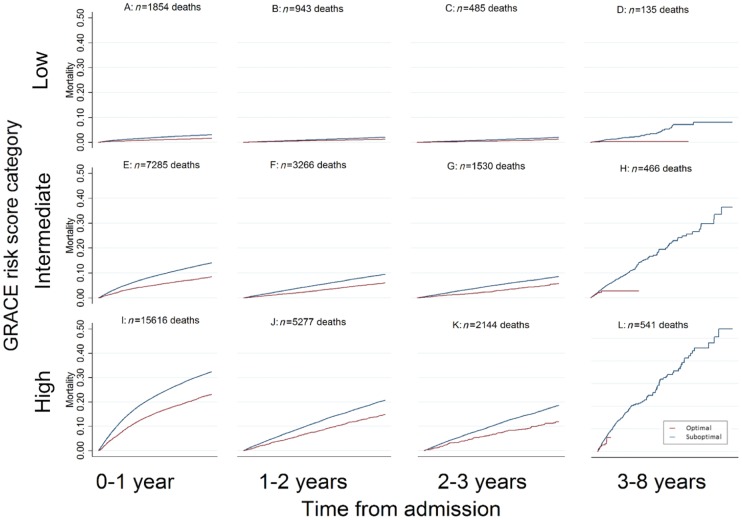
Methods and results: National cohort study (n = 389 507 patients, n = 232 hospitals, MINAP registry), 2003-2013. The primary outcome was adjusted all-cause survival estimated using flexible parametric survival modelling with time-varying covariates. Optimal care was defined as the receipt of all eligible treatments and was inversely related to risk status (defined by the GRACE risk score): 25.6% in low, 18.6% in intermediate, and 11.5% in high-risk NSTEMI. At 30 days, the use of optimal care was associated with improved survival among high [adjusted hazard ratio (aHR) -0.66 95% confidence interval (CI) 0.53-0.86, difference in absolute mortality rate (AMR) per 100 patients (AMR/100-0.19 95% CI -0.29 to -0.08)], and intermediate (aHR = 0.74, 95% CI 0.62-0.92; AMR/100 = -0.15, 95% CI -0.23 to -0.08) risk NSTEMI. At the end of follow-up (8.4 years, median 2.3 years), the significant association between the use of all eligible guideline-indicated treatments and improved survival remained only for high-risk NSTEMI (aHR = 0.66, 95% CI 0.50-0.96; AMR/100 = -0.03, 95% CI -0.06 to -0.01). For low-risk NSTEMI, there was no association between the use of optimal care and improved survival at 30 days (aHR = 0.92, 95% CI 0.69-1.38) and at 8.4 years (aHR = 0.71, 95% CI 0.39-3.74).
Conclusion: Optimal use of guideline-indicated care for NSTEMI was associated with greater survival gains with increasing GRACE risk, but its use decreased with increasing GRACE risk.
Figures
References
-
- Peterson ED, Roe MT, Mulgund J, DeLong ER, Lytle BL, Brindis RG, Smith SC, Pollack CV, Newby LK, Harrington RA, Gibler WB, Ohman EM.. Association between hospital process performance and outcomes among patients with acute coronary syndromes. JAMA 2006;295:1912–1920. - PubMed
-
- Dondo TB, Hall M, Timmis AD, Gilthorpe MS, Alabas OA, Batin PD, Deanfield JE, Hemingway H, Gale CP.. Excess mortality and guideline-indicated care following non-ST-elevation myocardial infarction. Eur Heart J Acute Cardiovasc Care 2017;6:412.. - PubMed
-
- Hall M, Dondo TB, Yan AT, Goodman SG, Bueno H, Chew DP, Brieger D, Timmis A, Batin PD, Deanfield JE, Hemingway H, Fox KAA, Gale CP.. Association of clinical factors and therapeutic strategies with improvements in survival following non–ST-elevation myocardial infarction, 2003-2013. JAMA 2016;316:1073–1082. - PubMed
-
- Zaman MJ, Stirling S, Shepstone L, Ryding A, Flather M, Bachmann M, Myint PK.. The association between older age and receipt of care and outcomes in patients with acute coronary syndromes: a cohort study of the Myocardial Ischaemia National Audit Project (MINAP). Eur Heart J 2014;35:1551–1558. - PubMed
-
- Mukherjee D, Fang J, Chetcuti S, Moscucci M, Kline-Rogers E, Eagle KA.. Impact of combination evidence-based medical therapy on mortality in patients with acute coronary syndromes. Circulation 2004;109:745–749. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
