

The Impact of Intensive Versus Standard Anthelminthic Treatment on Allergy-related Outcomes, Helminth Infection Intensity, and Helminth-related Morbidity in Lake Victoria Fishing Communities, Uganda: Results From the LaVIISWA Cluster-randomized Trial
- PMID: 30202872
- PMCID: PMC6495012
- DOI: 10.1093/cid/ciy761
The Impact of Intensive Versus Standard Anthelminthic Treatment on Allergy-related Outcomes, Helminth Infection Intensity, and Helminth-related Morbidity in Lake Victoria Fishing Communities, Uganda: Results From the LaVIISWA Cluster-randomized Trial
Abstract
Background: The prevalence of allergy-related diseases is increasing in low-income countries. Parasitic helminths, common in these settings, may be protective. We hypothesized that intensive, community-wide, anthelminthic mass drug administration (MDA) would increase allergy-related diseases, while reducing helminth-related morbidity.
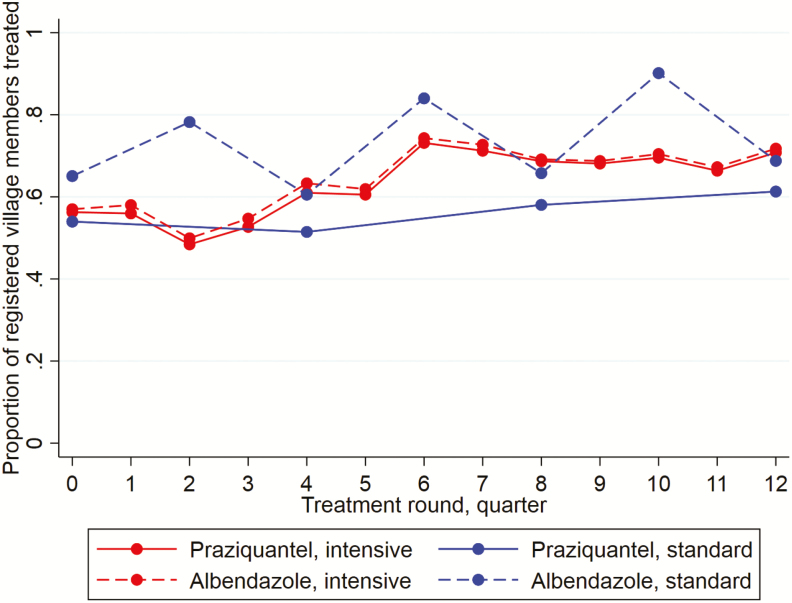
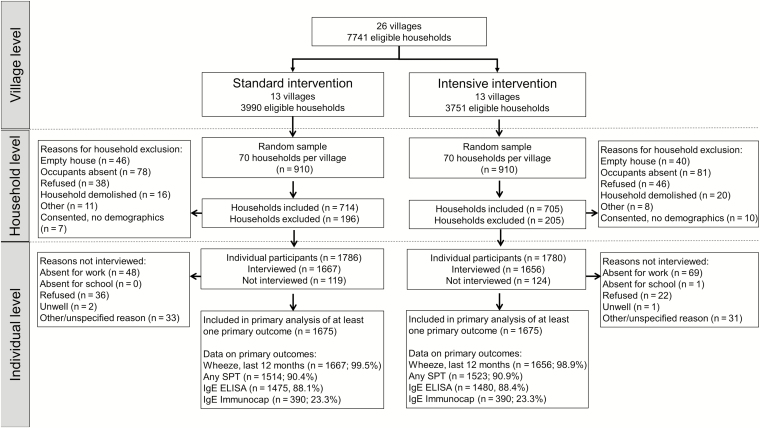
Methods: In an open, cluster-randomized trial (ISRCTN47196031), we randomized 26 high-schistosomiasis-transmission fishing villages in Lake Victoria, Uganda, in a 1:1 ratio to receive community-wide intensive (quarterly single-dose praziquantel plus albendazole daily for 3 days) or standard (annual praziquantel plus 6 monthly single-dose albendazole) MDA. Primary outcomes were recent wheezing, skin prick test positivity (SPT), and allergen-specific immunoglobulin E (asIgE) after 3 years of intervention. Secondary outcomes included helminths, haemoglobin, and hepatosplenomegaly.
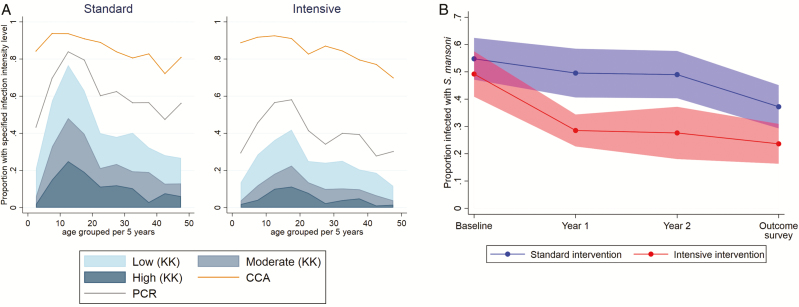
Results: The outcome survey comprised 3350 individuals. Intensive MDA had no effect on wheezing (risk ratio [RR] 1.11, 95% confidence interval [CI] 0.64-1.93), SPT (RR 1.10, 95% CI 0.85-1.42), or asIgE (RR 0.96, 95% CI 0.82-1.12). Intensive MDA reduced Schistosoma mansoni infection intensity: the prevalence from Kato Katz examinations of single stool samples from each patient was 23% versus 39% (RR 0.70, 95% CI 0.55-0.88), but the urine circulating cathodic antigen test remained positive in 85% participants in both trial arms. Hookworm prevalence was 8% versus 11% (RR 0.55, 95% CI 0.31-1.00). There were no differences in anemia or hepatospenomegaly between trial arms.
Conclusions: Despite reductions in S. mansoni intensity and hookworm prevalence, intensive MDA had no effect on atopy, allergy-related diseases, or helminth-related pathology. This could be due to sustained low-intensity infections; thus, a causal link between helminths and allergy outcomes cannot be discounted. Intensive community-based MDA has a limited impact in high-schistosomiasis-transmission fishing communities, in the absence of other interventions.
Clinical trials registration: ISRCTN47196031.
Keywords: Schistosoma mansoni; Africa; allergy-related disease; helminths; mass drug administration.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America.
Figures
References
-
- Nicolaou N, Siddique N, Custovic A. Allergic disease in urban and rural populations: increasing prevalence with increasing urbanization. Allergy 2005; 60:1357–60. - PubMed
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
