

Effects of positive end-expiratory pressure strategy in supine and prone position on lung and chest wall mechanics in acute respiratory distress syndrome
- PMID: 30203117
- PMCID: PMC6134472
- DOI: 10.1186/s13613-018-0434-2
Effects of positive end-expiratory pressure strategy in supine and prone position on lung and chest wall mechanics in acute respiratory distress syndrome
Abstract
Background: In acute respiratory distress syndrome (ARDS) patients, it has recently been proposed to set positive end-expiratory pressure (PEEP) by targeting end-expiratory transpulmonary pressure. This approach, which relies on the measurement of absolute esophageal pressure (Pes), has been used in supine position (SP) and has not been investigated in prone position (PP). Our purposes were to assess Pes-guided strategy to set PEEP in SP and in PP as compared with a PEEP/FIO2 table and to explore the early (1 h) and late (16 h) effects of PP on lung and chest wall mechanics.
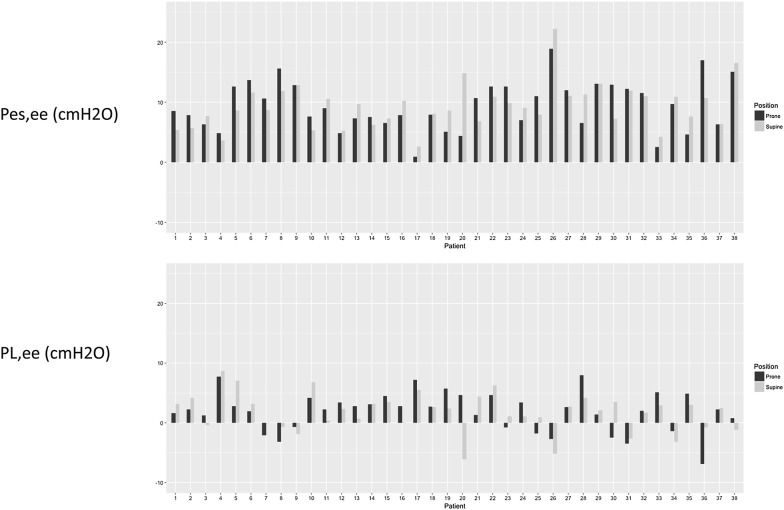
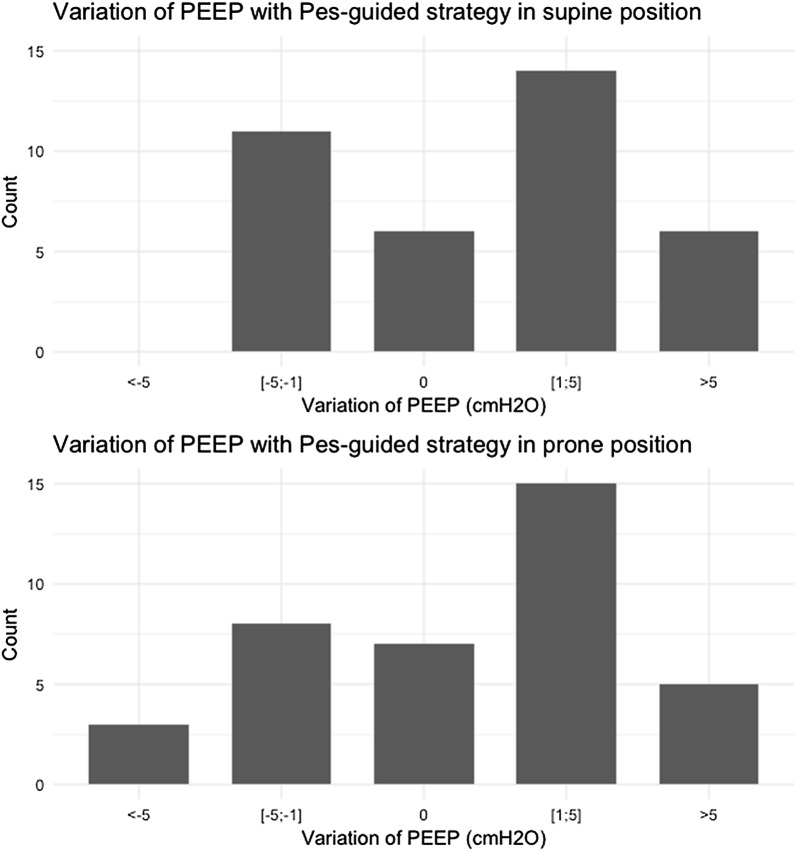
Results: We performed a prospective, physiologic study in two ICUs in university hospitals on ARDS patients with PaO2/FIO2 < 150 mmHg. End-expiratory Pes (Pes,ee) was measured in static (zero flow) condition. Patients received PEEP set according to a PEEP/FIO2 table then according to the Pes-guided strategy targeting a positive (3 ± 2 cmH2O) static end-expiratory transpulmonary pressure in SP. Then, patients were turned to PP and received same amount of PEEP from PEEP/FIO2 table then Pes-guided strategy. Respiratory mechanics, oxygenation and end-expiratory lung volume (EELV) were measured after 1 h of each PEEP in each position. For the rest of the 16-h PP session, patients were randomly allocated to either PEEP strategy with measurements done at the end. Thirty-eight ARDS patients (27 male), mean ± SD age 63 ± 13 years, were included. There were 33 primary ARDS and 26 moderate ARDS. PaO2/FIO2 ratio was 120 ± 23 mmHg. At same PEEP/FIO2 table-related PEEP, Pes,ee averaged 9 ± 4 cmH2O in both SP and PP (P = 0.88). With PEEP/FIO2 table and Pes-guided strategy, PEEP was 10 ± 2 versus 12 ± 4 cmH2O in SP and 10 ± 2 versus 12 ± 5 cmH2O in PP (PEEP strategy effect P = 0.05, position effect P = 0.96, interaction P = 0.96). With the Pes-guided strategy, chest wall elastance increased regardless of position. Lung elastance and transpulmonary driving pressure decreased in PP, with no effect of PEEP strategy. Both PP and Pes-guided strategy improved oxygenation without interaction. EELV did not change with PEEP strategy. At the end of PP session, respiratory mechanics did not vary but EELV and PaO2/FIO2 increased while PaCO2 decreased.
Conclusions: There was no impact of PP on Pes measurements. PP had an immediate improvement effect on lung mechanics and a late lung recruitment effect independent of PEEP strategy.
Keywords: Acute respiratory distress syndrome; Electrical impedance tomography; Esophageal pressure; Positive end-expiratory pressure; Prone position; Transpulmonary pressure.
Figures
References
-
- Meade MO, Cook DJ, Guyatt GH, Slutsky AS, Arabi YM, Cooper DJ, et al. Ventilation strategy using low tidal volumes, recruitment maneuvers, and high positive end-expiratory pressure for acute lung injury and acute respiratory distress syndrome: a randomized controlled trial. JAMA. 2008;299:637–645. doi: 10.1001/jama.299.6.637. - DOI - PubMed
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
