

Transverse debridement and acute shortening followed by distraction histogenesis in the treatment of open tibial fractures with bone and soft tissue loss
- PMID: 30203142
- PMCID: PMC6249147
- DOI: 10.1007/s11751-018-0316-z
Transverse debridement and acute shortening followed by distraction histogenesis in the treatment of open tibial fractures with bone and soft tissue loss
Abstract
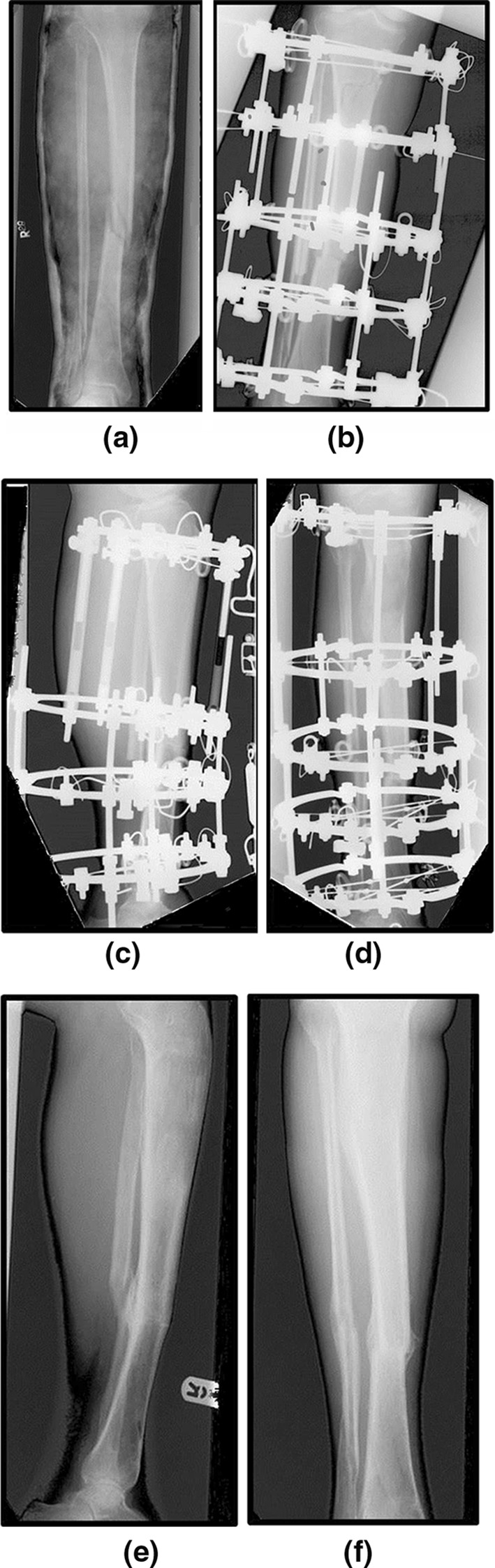
This retrospective case series evaluates the technique of transverse debridement, acute shortening and subsequent distraction histogenesis in the management of open tibial fractures with bone and soft tissue loss, thereby avoiding the need for a soft tissue flap to cover the wound. Thirty-one patients with Gustilo grade III open tibial fractures between 2001 and 2011 were initially managed with transverse wound extensions, debridement and shortening to provide bony apposition and allowing primary wound closure without tension, or coverage with mobilization of soft tissue and split skin graft. Temporary monolateral external fixation was used to allow soft tissues resuscitation, followed by Ilizarov frame for definitive fracture stabilization. Leg length discrepancy was corrected by corticotomy and distraction histogenesis. Union was evaluated radiologically and clinically. Patients' mean age was 37.3 years (18.3-59.3). Mean bone defect was 3.2 cm (1-8 cm). Mean time to union was 40.1 weeks (12.6-80.7 weeks), and median frame index was 75 days/cm. Median lengthening index (time in frame after corticotomy for lengthening) was 63 days/cm. Mean clinic follow-up was 79 weeks (23-174). Six patients had a total of seven complications. Four patients re-fractured after frame removal, one of whom required a second frame. Two patients required a second frame for correction of residual deformity, and one patient developed a stiff non-union which united following a second frame. There were no cases of deep infection. Acute shortening followed by distraction histogenesis is a safe method for the acute treatment of open tibial fractures with bone and soft tissue loss. This method also avoids the cost, logistical issues and morbidity associated with the use of local or free-tissue transfer flaps and has a low rate of serious complications despite the injury severity.
Keywords: Circular frame; Deformity correction; Distraction histogenesis; Ilizarov frame; Limb reconstruction; Open fractures; Soft tissue flap; Tibia.
Conflict of interest statement
Conflict of interest
The authors declare no conflict of interest.
Ethical standards
The work was registered with the host institution’s Clinical Effectiveness Unit, and no ethical approval is required.
Figures



References
-
- Nanchahal J, Nayagam D, et al. The standards for the management of open fractures of the lower limb. 1. London: Royal Society of Medicine Press Ltd; 2009.
LinkOut - more resources
Full Text Sources
Other Literature Sources
