

Myofascial trigger points in migraine and tension-type headache
- PMID: 30203398
- PMCID: PMC6134706
- DOI: 10.1186/s10194-018-0913-8
Myofascial trigger points in migraine and tension-type headache
Abstract
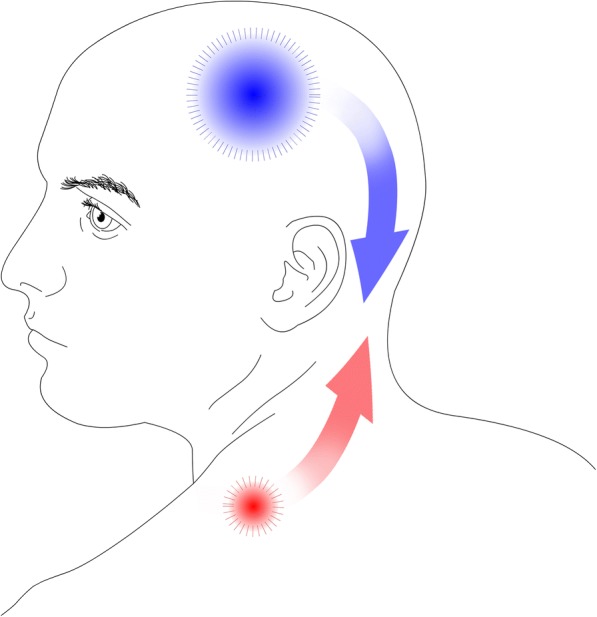
Background: A myofascial trigger point is defined as a hyperirritable spot in skeletal muscle that is associated with a hypersensitive palpable nodule in a taut band. It has been suggested that myofascial trigger points take part in chronic pain conditions including primary headache disorders. The aim of this narrative review is to present an overview of the current imaging modalities used for the detection of myofascial trigger points and to review studies of myofascial trigger points in migraine and tension-type headache.
Findings: Different modalities have been used to assess myofascial trigger points including ultrasound, microdialysis, electromyography, infrared thermography, and magnetic resonance imaging. Ultrasound is the most promising of these modalities and may be used to identify MTrPs if specific methods are used, but there is no precise description of a gold standard using these techniques, and they have yet to be evaluated in headache patients. Active myofascial trigger points are prevalent in migraine patients. Manual palpation can trigger migraine attacks. All intervention studies aiming at trigger points are positive, but this needs to be further verified in placebo-controlled environments. These findings may imply a causal bottom-up association, but studies of migraine patients with comorbid fibromyalgia syndrome suggest otherwise. Whether myofascial trigger points contribute to an increased migraine burden in terms of frequency and intensity is unclear. Active myofascial trigger points are prevalent in tension-type headache coherent with the hypothesis that peripheral mechanisms are involved in the pathophysiology of this headache disorder. Active myofascial trigger points in pericranial muscles in tension-type headache patients are correlated with generalized lower pain pressure thresholds indicating they may contribute to a central sensitization. However, the number of active myofascial trigger points is higher in adults compared with adolescents regardless of no significant association with headache parameters. This suggests myofascial trigger points are accumulated over time as a consequence of TTH rather than contributing to the pathophysiology.
Conclusions: Myofascial trigger points are prevalent in both migraine and tension-type headache, but the role they play in the pathophysiology of each disorder and to which degree is unclarified. In the future, ultrasound elastography may be an acceptable diagnostic test.
Keywords: Diagnostic test; Headache; Migraine; Muscle; Myofascial trigger point; Tension-type headache; Treatment; Trigemino-cervical-complex.
Conflict of interest statement
Ethics approval and consent to participate
Not applicable.
Consent for publication
Not applicable.
Competing interests
HWS has received travel grants or speaking fees from Pfizer, Autonomic Technologies and Novartis. TPD, GFH, LTK and JH declare that they have no competing interests.
Publisher’s Note
Springer Nature remains neutral with regard to jurisdictional claims in published maps and institutional affiliations.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
