

Human inner ear blood supply revisited: the Uppsala collection of temporal bone-an international resource of education and collaboration
- PMID: 30204028
- PMCID: PMC6198224
- DOI: 10.1080/03009734.2018.1492654
Human inner ear blood supply revisited: the Uppsala collection of temporal bone-an international resource of education and collaboration
Abstract
Background: The Uppsala collection of human temporal bones and molds is a unique resource for education and international research collaboration. Micro-computerized tomography (micro-CT) and synchrotron imaging are used to investigate the complex anatomy of the inner ear. Impaired microcirculation is etiologically linked to various inner ear disorders, and recent developments in inner ear surgery promote examination of the vascular system. Here, for the first time, we present three-dimensional (3D) data from investigations of the major vascular pathways and corresponding bone channels.
Methods: We used the archival Uppsala collection of temporal bones and molds consisting of 324 inner ear casts and 113 macerated temporal bones. Micro-CT was used to investigate vascular bone channels, and 26 fresh human temporal bones underwent synchrotron radiation phase contrast imaging (SR-PCI). Data were processed by volume-rendering software to create 3D reconstructions allowing orthogonal sectioning, cropping, and soft tissue analyses.
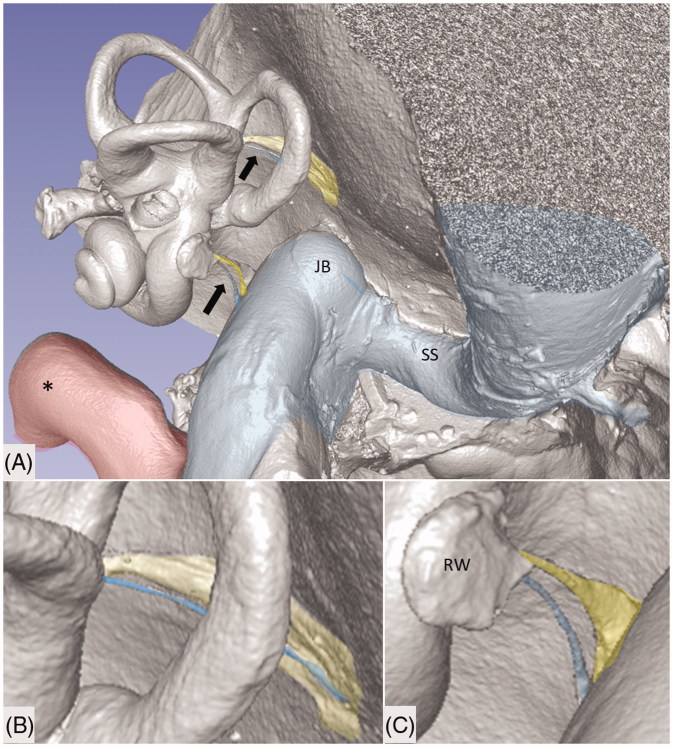
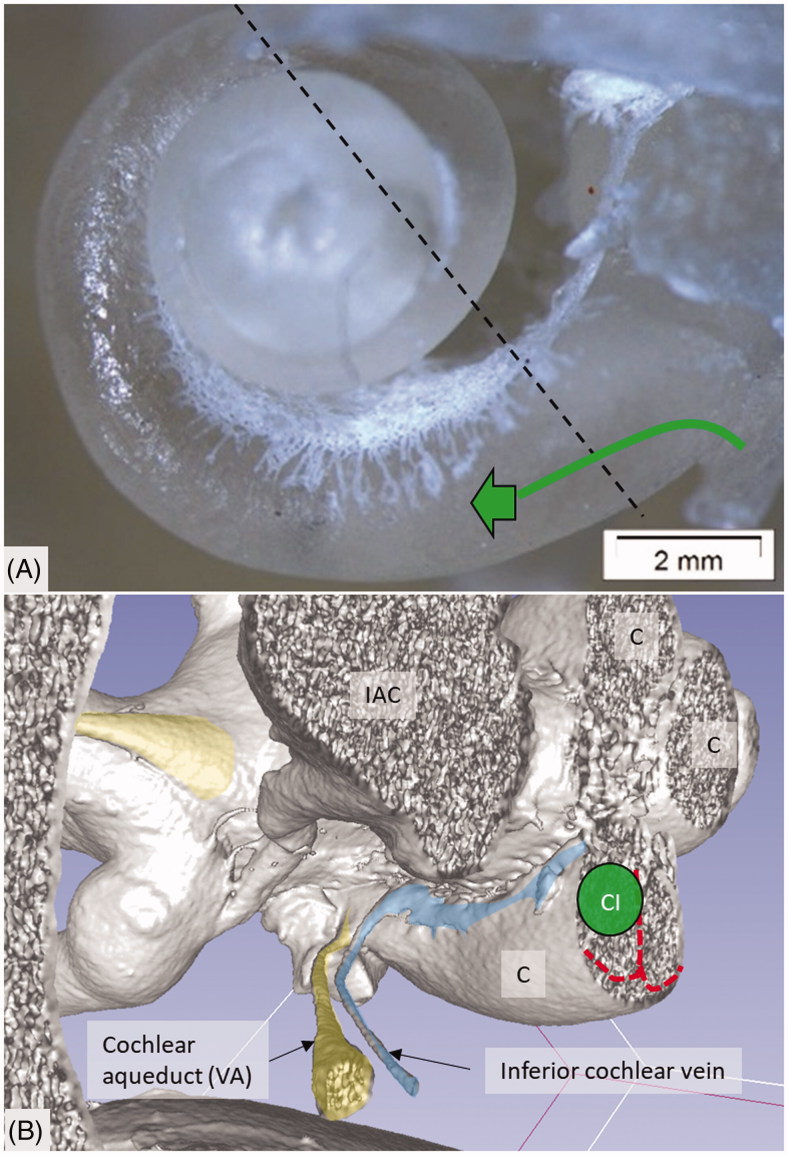
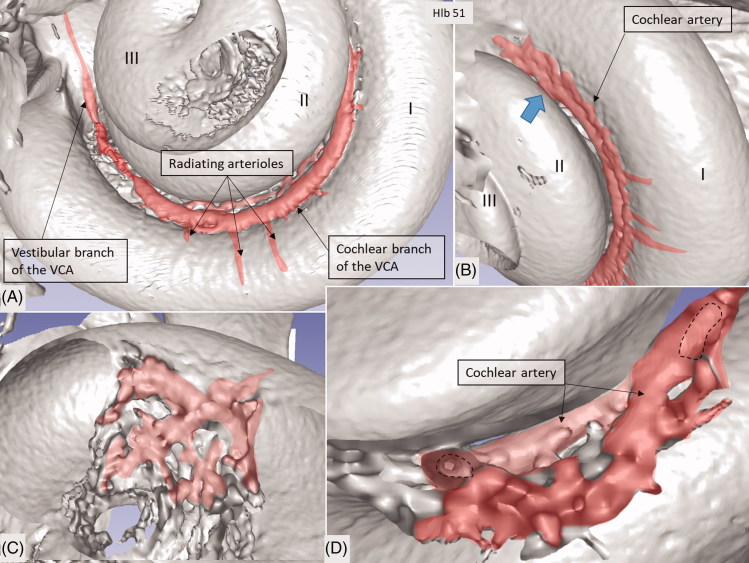
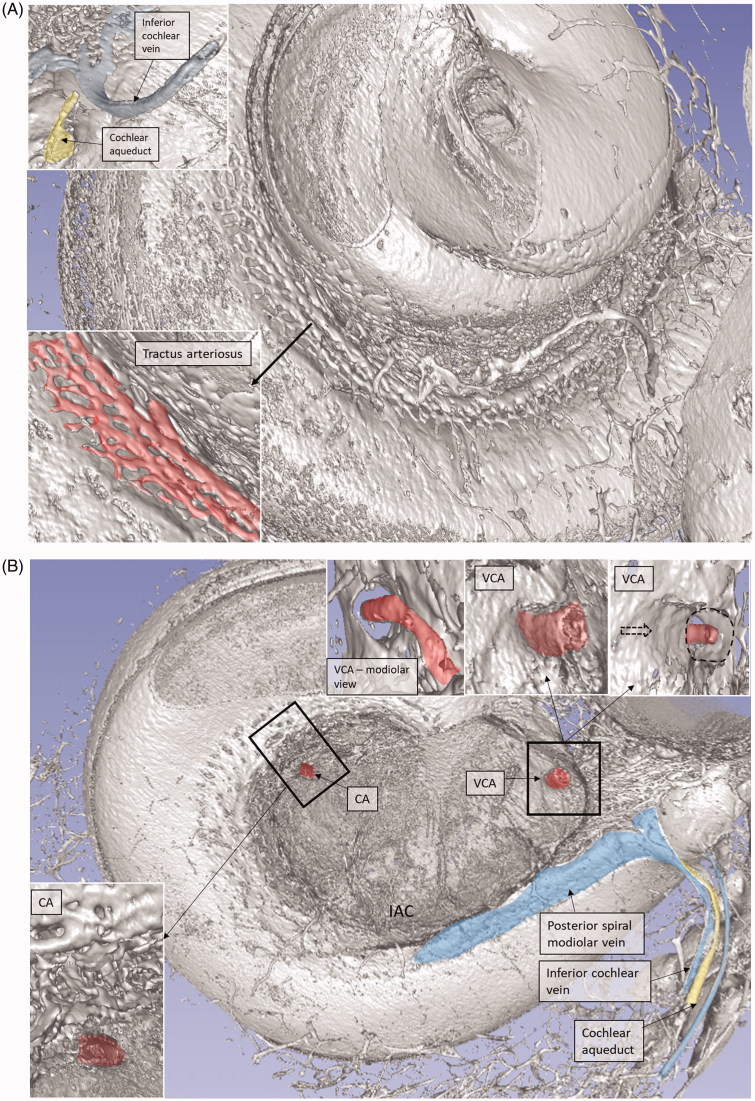
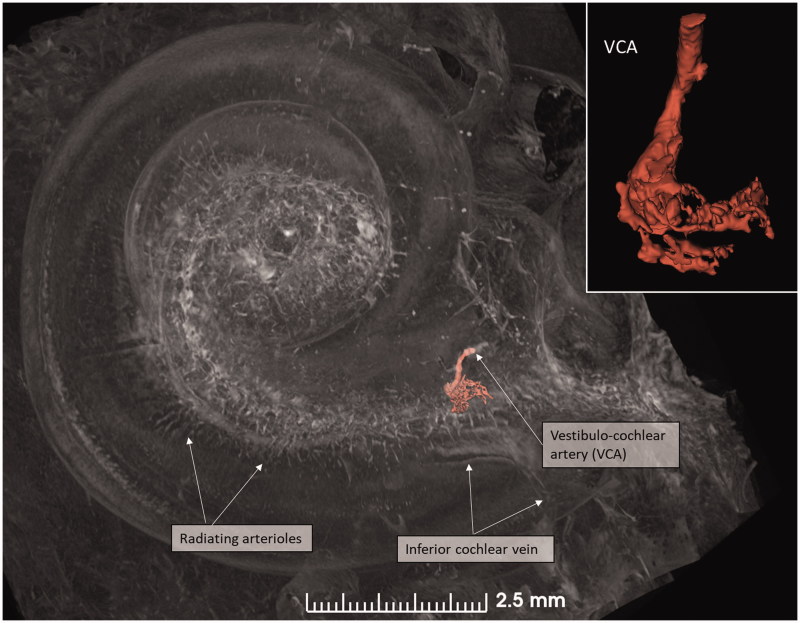
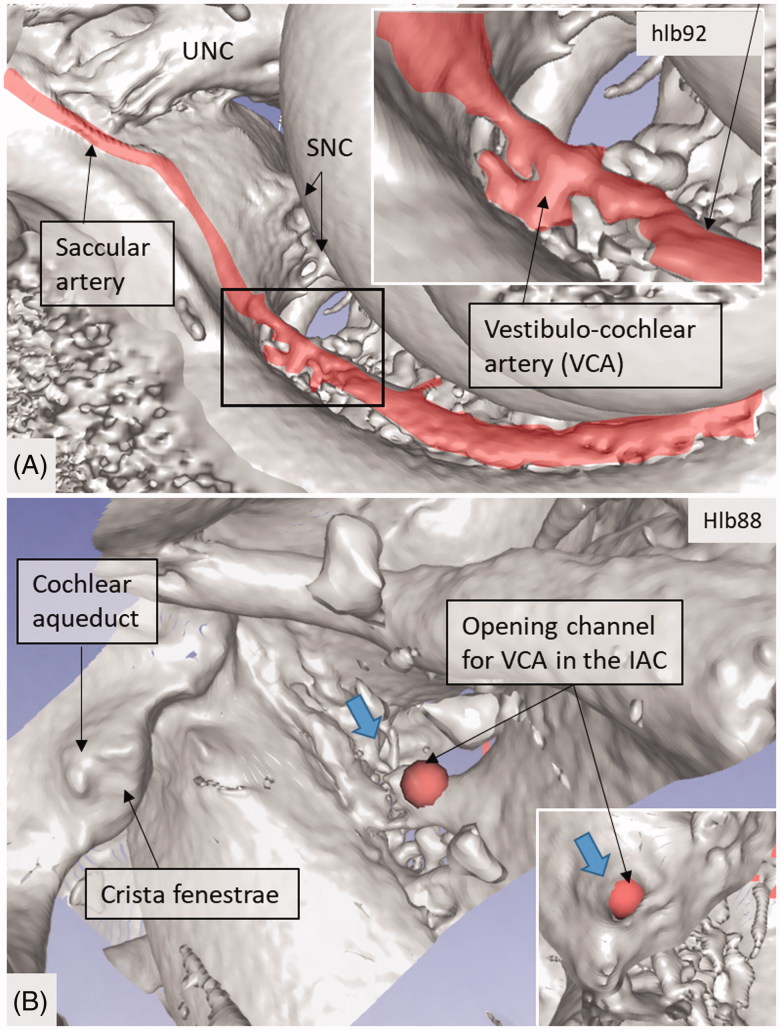
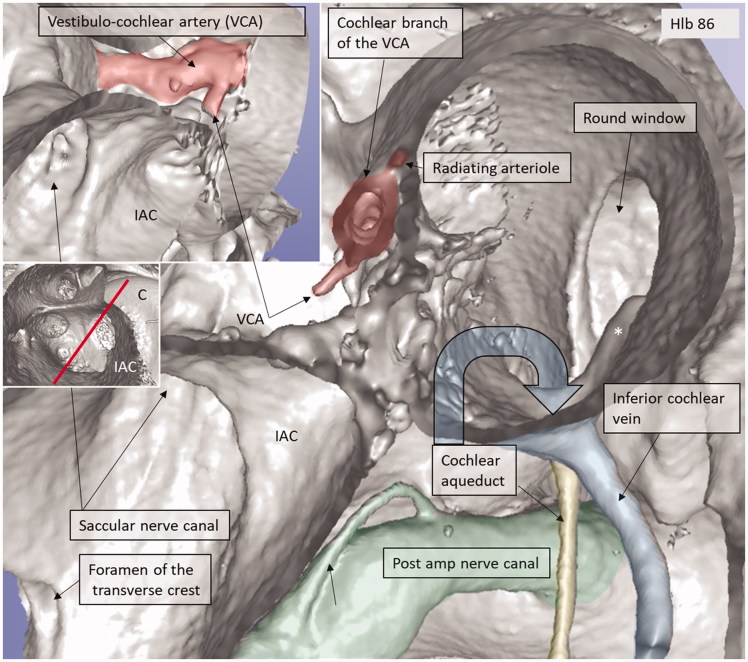
Results: Micro-CT with 3D rendering was superior in reproducing the anatomy of the vascular bone channels, while SR-PCI replicated soft tissues. Arterial bone channels were traced from scala vestibuli (SV) arterioles to the fundus, cochlea, and vestibular apparatus. Drainage routes along the aqueducts were examined.
Conclusion: Human inner ear vessels are difficult to study due to the adjoining hard bone. Micro-CT and SR-PCI with 3D reconstructions revealed large portions of the micro-vascular system in un-decalcified specimens. The results increase our understanding of the organization of the vascular system in humans and how altered microcirculation may relate to inner ear disorders. The findings may also have surgical implications.
Keywords: Human; Uppsala collection; micro-computerized tomography; synchrotron phase contrast imaging; temporal bone.
Figures
Similar articles
-
Improved middle-ear soft-tissue visualization using synchrotron radiation phase-contrast imaging.Hear Res. 2017 Oct;354:1-8. doi: 10.1016/j.heares.2017.08.001. Epub 2017 Aug 5. Hear Res. 2017. PMID: 28822316
-
Incus Necrosis and Blood Supply: A Micro-CT and Synchrotron Imaging Study.Otol Neurotol. 2019 Aug;40(7):e713-e722. doi: 10.1097/MAO.0000000000002292. Otol Neurotol. 2019. PMID: 31135670
-
Three-dimensional imaging of the human internal acoustic canal and arachnoid cistern: a synchrotron study with clinical implications.J Anat. 2019 Mar;234(3):316-326. doi: 10.1111/joa.12926. Epub 2018 Dec 18. J Anat. 2019. PMID: 30565214 Free PMC article.
-
Special Anatomic Considerations in Otosclerosis Surgery.Otolaryngol Clin North Am. 2018 Apr;51(2):357-374. doi: 10.1016/j.otc.2017.11.013. Epub 2018 Feb 1. Otolaryngol Clin North Am. 2018. PMID: 29397114 Review.
-
Middle and inner ear: improved depiction with multiplanar reconstruction of volumetric CT data.Radiographics. 2006 Jan-Feb;26(1):115-24. doi: 10.1148/rg.261055703. Radiographics. 2006. PMID: 16418247 Review.
Cited by
-
Prognosis of vestibular dysfunction in idiopathic sudden sensorineural hearing loss with vertigo: a prospective cohort study.J Neurol. 2023 Nov;270(11):5516-5526. doi: 10.1007/s00415-023-11894-w. Epub 2023 Jul 30. J Neurol. 2023. PMID: 37517037
-
Histopathological changes to the peripheral vestibular system following meningitic labyrinthitis.Laryngoscope Investig Otolaryngol. 2020 Feb 14;5(2):256-266. doi: 10.1002/lio2.349. eCollection 2020 Apr. Laryngoscope Investig Otolaryngol. 2020. PMID: 32337357 Free PMC article.
-
Five consecutive cases of sensorineural hearing loss associated with inner ear barotrauma due to diving, successfully treated with hyperbaric oxygen.Diving Hyperb Med. 2024 Dec 20;54(4):360-367. doi: 10.28920/dhm54.4.360-367. Diving Hyperb Med. 2024. PMID: 39675746
-
Cardiovascular risk factors among patients with acute unilateral inner ear hypofunction: A case-control study.Laryngoscope Investig Otolaryngol. 2022 Dec 12;8(1):245-252. doi: 10.1002/lio2.992. eCollection 2023 Feb. Laryngoscope Investig Otolaryngol. 2022. PMID: 36846399 Free PMC article.
-
Investigations of the Microvasculature of the Human Macula Utricle in Meniere's Disease.Front Cell Neurosci. 2019 Oct 4;13:445. doi: 10.3389/fncel.2019.00445. eCollection 2019. Front Cell Neurosci. 2019. PMID: 31636542 Free PMC article.
References
-
- Wilbrand HF, Rask-Andersen H, Gilstring D. The vestibular aqueduct and the para-vestibular canal. An anatomic and roentgenologic investigation. Acta Radiol Diagn (Stockh). 1974;15:337–55. - PubMed
-
- Rask-Andersen H, Stahle J, Wilbrand H. Human cochlear aqueduct and its accessory canals. Ann Otol Rhinol Laryngol Suppl. 1977;86:1–16. - PubMed
-
- Wadin K. Imaging contributions to the temporal bone anatomy (high jugular fossae). Scand Audiol Suppl. 1988;30:145–8. - PubMed
-
- Siebenmann F. Die Korrosionsanatomie des knöchernen Labyrinthes des menschlichen Ohres. Wiesbaden, Germany: C. F. Bergmann; 1890.
-
- Siebenmann F. Die Blutgefässa des Labyrinthes des menschlichen Ohres. Wiesbaden, Germany: C. F. Bergmann; 1894.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous