

Dual-Energy CT Angiography for Detection of Pulmonary Emboli: Incremental Benefit of Iodine Maps
- PMID: 30204073
- PMCID: PMC6209063
- DOI: 10.1148/radiol.2018180594
Dual-Energy CT Angiography for Detection of Pulmonary Emboli: Incremental Benefit of Iodine Maps
Abstract
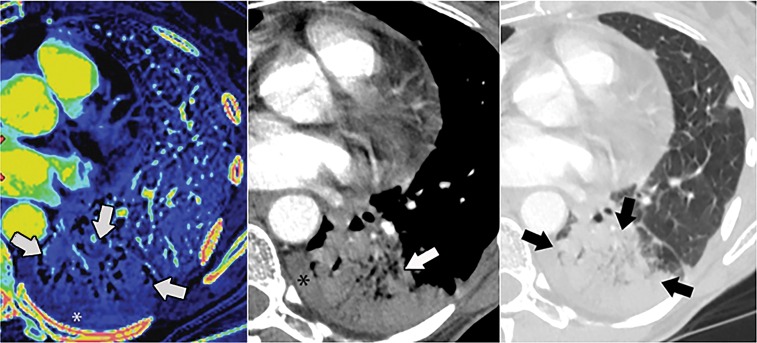
Purpose To determine if there is added benefit of using iodine maps from dual-energy (DE) CT in addition to conventional CT angiography images to diagnose pulmonary embolism (PE). Materials and Methods In this retrospective analysis, 1144 consecutive dual-energy CT angiography examinations performed from January through September 2014 at an oncologic referral center to evaluate for PE were reviewed. The 1144 examinations included 1035 patients (mean age, 58.7 years; range, 15-99 years). First, the location, level, and type (occlusive vs nonocclusive) of PEs on conventional CT angiograms were recorded. Iodine maps were then reviewed for defects suggestive of PE. Last, CT angiograms were rereviewed to detect additional PEs suggested by the iodine map. Consensus reviews were performed for examinations with PEs. The confidence interval of percentages was calculated by using the Clopper-Pearson method. Results On 147 of 1144 (12.8%) CT angiograms, a total of 372 PEs were detected at initial review. After review of the DE CT iodine map, 27 additional PEs were found on 26 of 1144 CT angiograms (2.3%; 95% confidence interval [CI]: 1.5%, 3.3%). Of the 27 additional PEs, six (22.2%) were segmental, 21 (77.8%) were subsegmental, 24 (88.9%) were occlusive, and three (11.1%) were nonocclusive. Eleven of 1144 (1.0%; 95% CI: 0.5%, 1.7%) CT angiograms had a new diagnosis of PE after review of the DE CT iodine maps. Conclusion Dual-energy CT iodine maps show a small incremental benefit for the detection of occlusive segmental and subsegmental pulmonary emboli. © RSNA, 2018.
Figures




Similar articles
-
State of the art: utility of multi-energy CT in the evaluation of pulmonary vasculature.Int J Cardiovasc Imaging. 2019 Aug;35(8):1509-1524. doi: 10.1007/s10554-019-01615-8. Epub 2019 May 2. Int J Cardiovasc Imaging. 2019. PMID: 31049753 Review.
-
Iodine Maps from Subtraction CT or Dual-Energy CT to Detect Pulmonary Emboli with CT Angiography: A Multiple-Observer Study.Radiology. 2019 Jul;292(1):197-205. doi: 10.1148/radiol.2019182666. Epub 2019 May 14. Radiology. 2019. PMID: 31084482
-
Evaluation of pulmonary embolism in pediatric patients with nephrotic syndrome with dual energy CT pulmonary angiography.Acad Radiol. 2012 Mar;19(3):341-8. doi: 10.1016/j.acra.2011.11.002. Epub 2011 Dec 15. Acad Radiol. 2012. PMID: 22177283
-
Iodine Distribution Map in Dual-Energy Computed Tomography Pulmonary Artery Imaging with Rapid kVp Switching for the Diagnostic Analysis and Quantitative Evaluation of Acute Pulmonary Embolism.Acad Radiol. 2015 Jun;22(6):743-51. doi: 10.1016/j.acra.2015.01.012. Epub 2015 Mar 13. Acad Radiol. 2015. PMID: 25772582
-
State-of-the-Art Pulmonary CT Angiography for Acute Pulmonary Embolism.AJR Am J Roentgenol. 2017 Mar;208(3):495-504. doi: 10.2214/AJR.16.17202. Epub 2016 Nov 29. AJR Am J Roentgenol. 2017. PMID: 27897042 Review.
Cited by
-
Dual-Energy Heart CT: Beyond Better Angiography-Review.J Clin Med. 2021 Nov 7;10(21):5193. doi: 10.3390/jcm10215193. J Clin Med. 2021. PMID: 34768713 Free PMC article. Review.
-
Accuracy of registration algorithms in subtraction CT of the lungs: A digital phantom study.Med Phys. 2019 May;46(5):2264-2274. doi: 10.1002/mp.13496. Epub 2019 Apr 8. Med Phys. 2019. PMID: 30888690 Free PMC article.
-
State of the art: utility of multi-energy CT in the evaluation of pulmonary vasculature.Int J Cardiovasc Imaging. 2019 Aug;35(8):1509-1524. doi: 10.1007/s10554-019-01615-8. Epub 2019 May 2. Int J Cardiovasc Imaging. 2019. PMID: 31049753 Review.
-
Spectral optimization using fast kV switching and filtration for photon counting CT with realistic detector responses: a simulation study.J Med Imaging (Bellingham). 2024 Dec;11(Suppl 1):S12805. doi: 10.1117/1.JMI.11.S1.S12805. Epub 2024 Jul 25. J Med Imaging (Bellingham). 2024. PMID: 39072221 Free PMC article.
-
Pulmonary Functional Imaging: Part 2-State-of-the-Art Clinical Applications and Opportunities for Improved Patient Care.Radiology. 2021 Jun;299(3):524-538. doi: 10.1148/radiol.2021204033. Epub 2021 Apr 13. Radiology. 2021. PMID: 33847518 Free PMC article. Review.
References
-
- Simonneau G, Sors H, Charbonnier B, et al. A comparison of low-molecular-weight heparin with unfractionated heparin for acute pulmonary embolism. The THESEE Study Group. Tinzaparine ou Heparine Standard: Evaluations dans l’Embolie Pulmonaire. N Engl J Med 1997;337(10):663–669. - PubMed
-
- Goldhaber SZ, Visani L, De Rosa M. Acute pulmonary embolism: clinical outcomes in the International Cooperative Pulmonary Embolism Registry (ICOPER). Lancet 1999;353(9162):1386–1389. - PubMed
-
- Baile EM, King GG, Müller NL, et al. . Spiral computed tomography is comparable to angiography for the diagnosis of pulmonary embolism. Am J Respir Crit Care Med 2000;161(3 Pt 1):1010–1015. - PubMed
-
- Hess S, Frary EC, Gerke O, Madsen PH. State-of-the-art imaging in pulmonary embolism: ventilation/perfusion single-photon emission computed tomography versus computed tomography angiography - controversies, results, and recommendations from a systematic review. Semin Thromb Hemost 2016;42(8):833–845. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
