

Transmission of Mobile Colistin Resistance (mcr-1) by Duodenoscope
- PMID: 30204838
- PMCID: PMC10849062
- DOI: 10.1093/cid/ciy683
Transmission of Mobile Colistin Resistance (mcr-1) by Duodenoscope
Abstract
Background: Clinicians increasingly utilize polymyxins for treatment of serious infections caused by multidrug-resistant gram-negative bacteria. Emergence of plasmid-mediated, mobile colistin resistance genes creates potential for rapid spread of polymyxin resistance. We investigated the possible transmission of Klebsiella pneumoniae carrying mcr-1 via duodenoscope and report the first documented healthcare transmission of mcr-1-harboring bacteria in the United States.
Methods: A field investigation, including screening targeted high-risk groups, evaluation of the duodenoscope, and genome sequencing of isolated organisms, was conducted. The study site included a tertiary care academic health center in Boston, Massachusetts, and extended to community locations in New England.
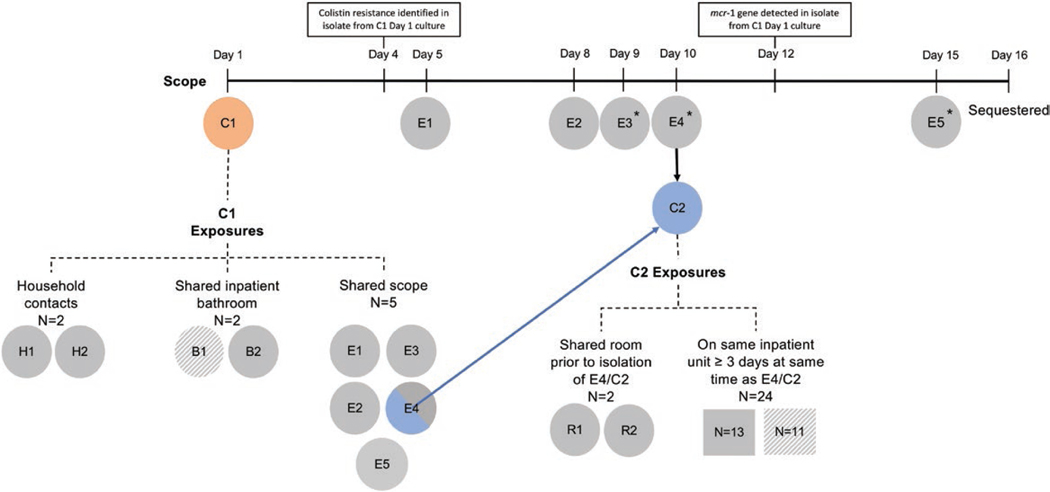
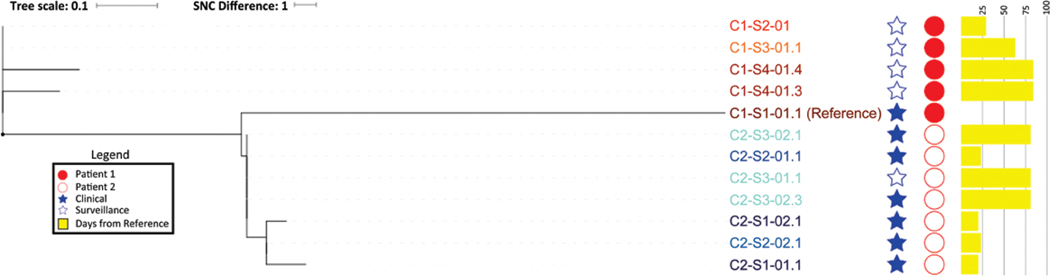
Results: Two patients had highly related mcr-1-positive K. pneumoniae isolated from clinical cultures; a duodenoscope was the only identified epidemiological link. Screening tests for mcr-1 in 20 healthcare contacts and 2 household contacts were negative. Klebsiella pneumoniae and Escherichia coli were recovered from the duodenoscope; neither carried mcr-1. Evaluation of the duodenoscope identified intrusion of biomaterial under the sealed distal cap; devices were recalled to repair this defect.
Conclusions: We identified transmission of mcr-1 in a United States acute care hospital that likely occurred via duodenoscope despite no identifiable breaches in reprocessing or infection control practices. Duodenoscope design flaws leading to transmission of multidrug-resistant organsisms persist despite recent initiatives to improve device safety. Reliable detection of colistin resistance is currently challenging for clinical laboratories, particularly given the absence of a US Food and Drug Administration-cleared test; improved clinical laboratory capacity for colistin susceptibility testing is needed to prevent the spread of mcr-carrying bacteria in healthcare settings.
Keywords: Klebsiella pneumoniae; duodenoscope; infection control; medical device safety; mobile colistin resistance.
© The Author(s) 2018. Published by Oxford University Press for the Infectious Diseases Society of America. All rights reserved. For permissions, e-mail: journals.permissions@oup.com.
Conflict of interest statement
Figures
References
-
- Seoane-Vazquez E, Rodriguez-Monguio R. Endoscopy-related infection: relic of the past? Curr Opin Infect Dis 2008; 21:362–6. - PubMed
-
- Srinivasan A. Epidemiology and prevention of infections related to endoscopy. Curr Infect Dis Rep 2003; 5:467–72. - PubMed
-
- Wendorf KA, Kay M, Baliga C, et al.. Endoscopic retrograde cholangiopancreatography-associated AmpC Escherichia coli outbreak. Infect Control Hosp Epidemiol 2015; 36:634–42. - PubMed
-
- Yang S, Hemarajata P, Hindler J, et al. Evolution and transmission of carbapenem-resistant Klebsiella pneumoniae expressing the blaOXA-232 gene during an institutional outbreak associated with endoscopic retrograde cholangiopancreatography. Clin Infect Dis 2017; 64:894–901. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
