

Efficacy of Nutritional Intervention in Elderly After Hip Fracture: A Multicenter Randomized Controlled Trial
- PMID: 30204859
- PMCID: PMC6132112
- DOI: 10.1093/gerona/gly030
Efficacy of Nutritional Intervention in Elderly After Hip Fracture: A Multicenter Randomized Controlled Trial
Abstract
Background: Malnutrition after hip fracture is associated with increased rehabilitation time, complications, and mortality. We assessed the effect of intensive 3 month nutritional intervention in elderly after hip fracture on length of stay (LOS).
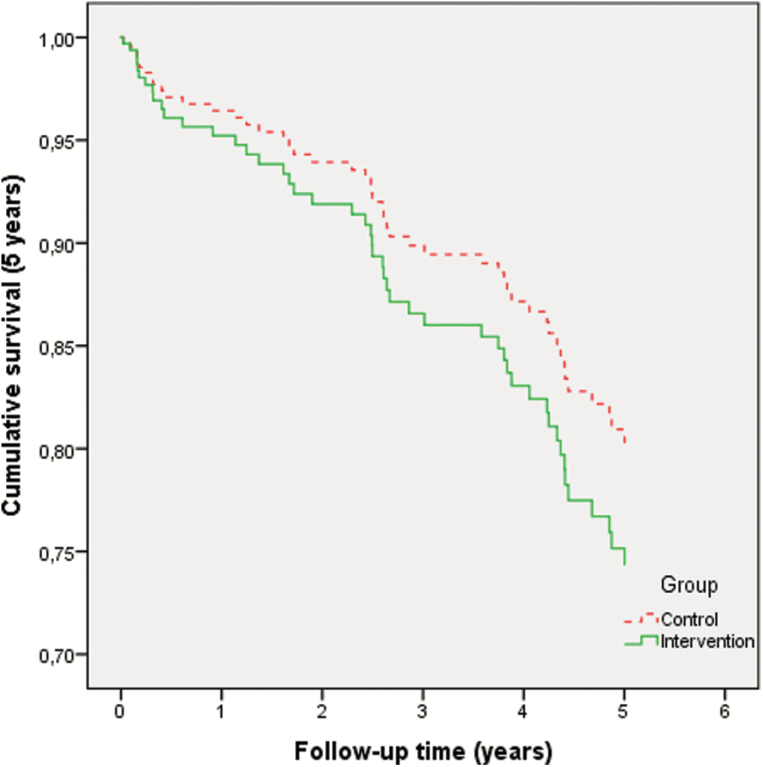
Methods: Open-label, randomized controlled trial. Exclusion criteria: age < 55 years, bone disease, life expectancy < 1 year, bedridden, using oral nutritional supplements (ONS) before hospitalization, and cognitive impairment. Intervention: weekly dietetic consultation, energy-protein-enriched diet, and ONS (400 mL per day) for 3 months. Control: usual nutritional care. Primary outcome: total LOS in hospital and rehabilitation clinic, including readmissions over 6 months (Cox regression adjusted for confounders); hazard ratio (HR) < 1.0 reflects longer LOS in the intervention group. Secondary outcomes: nutritional and functional status, cognition, quality of life, postoperative complications (6 months); subsequent fractures and all-cause mortality (1 and 5 years). Effect modification by baseline nutritional status was also tested.
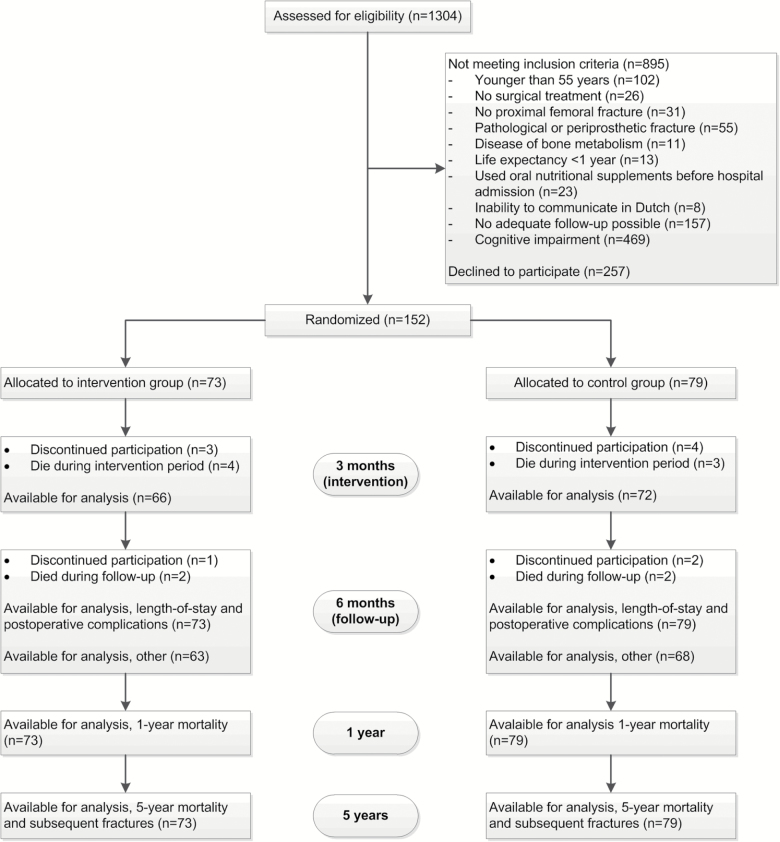
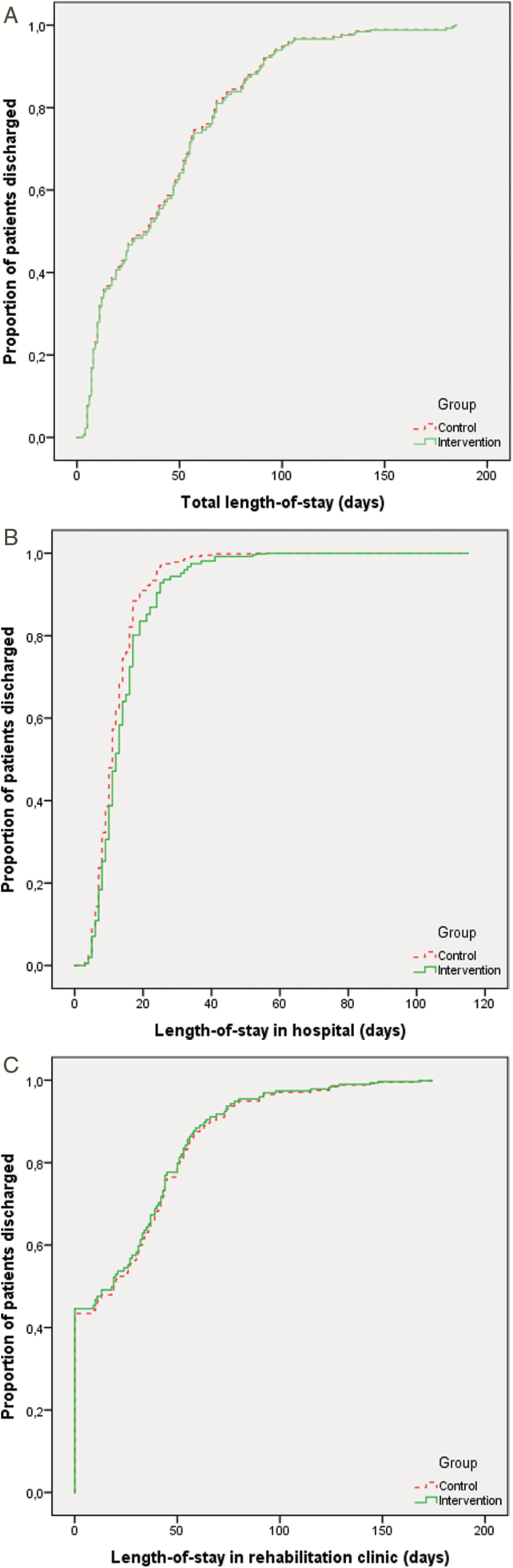
Results: One hundred fifty-two patients were randomized (73 intervention, 79 control). Median total LOS was 34.0 days (range 4-185 days) in the intervention group versus control 35.5 days (3-183 days; plogrank = .80; adjusted hazard ratio (adjHR): 0.98; 95% CI: 0.68-1.41). Hospital LOS: 12.0 days (4-56 days) versus 11.0 days (3-115 days; p = .19; adjHR: 0.75; 95% CI: 0.53-1.06) and LOS in rehabilitation clinics: 19.5 days (0-174 days) versus 18.5 days (0-168 days; p = .82; adjHR: 1.04; 95% CI: 0.73-1.48). The intervention improved nutritional intake/status at 3, but not at 6 months, and did not affect any other outcome. No difference in intervention effect between malnourished and well-nourished patients was found.
Conclusions: Intensive nutritional intervention after hip fracture improved nutritional intake and status, but not LOS or clinical outcomes. Paradigms underlying nutritional intervention in elderly after hip fracture may have to be reconsidered.
Trial registration: ClinicalTrials.gov NCT00523575.
Figures
Comment in
-
JPEN Journal Club 39. Validating a Surrogate.JPEN J Parenter Enteral Nutr. 2019 Jan;43(1):170-172. doi: 10.1002/jpen.1456. Epub 2018 Oct 9. JPEN J Parenter Enteral Nutr. 2019. PMID: 30299547 No abstract available.
References
-
- Cumming RG, Klineberg R, Katelaris A. Cohort study of risk of institutionalisation after hip fracture. Aust N Z J Public Health. 1996;20:579–582. doi:10.1111/j.1467-842X.1996.tb01069.x - PubMed
-
- Foster MR, Heppenstall RB, Friedenberg ZB, Hozack WJ. A prospective assessment of nutritional status and complications in patients with fractures of the hip. J Orthop Trauma. 1990;4:49–57. - PubMed
-
- Hernlund E, Svedbom A, Ivergård M et al. Osteoporosis in the European Union: medical management, epidemiology and economic burden. A report prepared in collaboration with the International Osteoporosis Foundation (IOF) and the European Federation of Pharmaceutical Industry Associations (EFPIA). Arch Osteoporos. 2013;8:136. doi:10.1007/s11657-013-0136-1 - PMC - PubMed
-
- Lumbers M, New SA, Gibson S, Murphy MC. Nutritional status in elderly female hip fracture patients: comparison with an age-matched home living group attending day centres. Br J Nutr. 2001;85:733–740. doi:10.1079/BJN2001350 - PubMed
-
- Delmi M, Rapin CH, Bengoa JM, Delmas PD, Vasey H, Bonjour JP. Dietary supplementation in elderly patients with fractured neck of the femur. Lancet. 1990;335:1013–1016. doi:10.1016/0140-6736(90)91073-J - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
